

Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Evaluations of phylogenetic proximity in a group of 67 dogs with
osteosarcoma: a pilot study
Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Canine Periosteal Osteosarcoma
Images added / Abbildungen hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
New subcategory added / Neue Unterkategorie hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
Images added / Abbildungen hinzugefügt 01.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Heart valvular diseases











The ultrasonography as an assistance to diagnostic of cholecystitis in a canine

Corina F Guendulain 1 *, MV; Griselda Gonzalez M 1 MV, Cl Cs Eng Vet; Carmen I Maffrand 2 MV, Cl Cs Eng Vet.
Small Animal Clinic 1 and 2 Clinical Laboratory Analysis, Animal Clinic Department, College of Agriculture and Veterinary Medicine, National University of Río Cuarto. Ruta 36 Km 601, Rio Cuarto, Cordoba, Argentina.
(Received: May 26, 2009 Accepted: January 19, 2010)

Summary
The cholecystitis is a gall-bladder inflamatory patology, the biliary obstruction and infection Could be the main causes of presentation. The diagnosis is dificult Because the clinical signs are inespecifics clinicopatological as abnormalities, so the Important ultrasonography is a method of diagnosis, the visualization of thickeny Because of the gall-bladder's wall leads to bile hiperecogenic or suspect cholecystitis. The bile culture and sensitivity testing permit to define the specific antibiotic treatment. A clinic case is Described to Emphasize The Importance of ultrasonography in the canine cholecystitis diagnosis.
Introduction
The canine cholecystitis is a rare inflammatory disease that affects the gallbladder (VB) and sometimes associated ducts. Although the pathogenesis of this entity is uncertain, biliary obstruction and infection would be the main causes of their presentation, entering enterobacteria retrograde through the common bile duct, or hematogenously from the adjacent hepatic circulation (Averis, 1996; Fossum and Willard, 1997; Strombeck and Guilford, 1995). Gram negative aerobic bacteria such as Escherichia coli, Klebsiella, Enterobacter, Proteus and Pseudomonas, are the most frequently isolated in canine bacterial cholecystitis but can also be found anaerobic bacteria such as Clostridium spp (Oswald et al., 1999).
The use of immunosuppressive drugs and certain systemic diseases such as diabetes mellitus, enteritis, septicemia, liver disease, biliary stasis, etc. They have been incriminated in the pathogenesis of cholecystitis, because favoring bacterial colonization of the gallbladder. Infection can result in necrosis and vesicular rupture if the bacteria damage the wall, cholangitis / colangiohepatitis amount if the biliary tree within the liver, or if emphysematous cholecystitis are gas producers (Fossum and Willard, 1997). Clinical signs are nonspecific, often have cranial abdominal pain, pyrexia, anorexia and vomiting, jaundice being one of the most common manifestations resulting from extrahepatic cholestasis due to decreased motility of the gallbladder, or abnormal bile components cholelithiasis (Fossum and Willard, 1997; Oswald et al, 1999)..
The hematology reveals a variety of nonspecific abnormalities such as anemia, leukocytosis and blood biochemistry in general demonstrates a commitment hepatobiliary system with increased alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma glutamyl transferase (GGT), alkaline phosphatase (FA), bilirubin, and cholesterol. In urinalysis can be bilirubinuria (Kaneko et al., 1997; Oswald et al., 1999; Smith and Biller, 2001). Ultrasound is the preferred technique for imagenological initial observation of the gallbladder and biliary tree, because it is noninvasive, is fast and safe (Smith and Biller, 2001). Ultrasound of the biliary system is indicated to rule out extrahepatic obstruction in jaundiced animals detect biliary calculi or masses and display wall thickening of the gallbladder. It is also useful to distinguish biliary obstruction of hepatocellular disease when serum biochemistry data are equivocal (Kaneko et al., 1997; Nyland and Mattoon, 2004).
Sonographically normal gallbladder is identified as an anechoic pear shaped structure surrounded by the hepatic parenchyma and located to the right of the midline. Has a thin wall thickness of 2-3 mm, which can be seen as a thin line between the anechoic echogenic bile and liver parenchyma, or not visible at all (Barr, 1992; Fritsch and Gerwing., 1996; Loriot et al, 1997; Nyland and Mattoon, 2004). Its size is variable and depends on the time of the last intake observed in anorexic animals a significant strain. Bile is hypoechoic normal due to the presence of corpuscular elements settle at rest; This sediment or biliary sludge tends to be located in the area of the bladder decline and produces acoustic shadow. This ultrasound finding usually indicates some degree of stasis and usually is little clinical significance unless the animal has obvious signs of obstruction (Fritsch and Gerwing, 1996; Jain, 1993, Loriot et al., 1997; Nyland and Mattoon , 2004). The cystic duct and the hepatic ducts are not detectable in normal animals and the bile appears as a hypoechoic tubular structure ventral portal vein, with a diameter less than 3 mm in dogs (Smith and biller, 2001). Biliary obstruction should be suspected when the bile overcomes these measures, or when the cystic duct or dilated bile ducts (Smith and biller, 2001) are.
Ultrasound is the method of choice to investigate vesicular changes, as both signs and physical findings are nonspecific. In cholecystitis VB walls are thickened and hyperechogenic. Although this finding is nonspecific, because it can be associated with multiple causes, such as acute hepatitis or chronic colangiohepatitis or chronic cholecystitis, it is suggestive of cholecystitis when it coexists with other clinical disorders (Nyland and Mattoon, 2004; Smith and biller, 2001 ). There may also be clay with or without bile coletitos, and edema, where the inner and outer walls become visible effect producing a double ring (Barr, 1992; Nyland and Mattoon, 2004).
Ultrasound can also see if abnormalities of the gallbladder, there are alterations in the liver parenchyma, thus allowing to make the distinction between pure and colangiohepatitis cholecystitis. Because these ultrasound findings do not serve to determine the etiology, it is necessary to resort to biopsy for diagnosis defi nite (Loriot et al., 1997). The ultrasound-guided percutaneous colecistocentesis to perform cytology and bile culture for aerobic and anaerobic bacteria, allows the identification of the causative agent and the selection of the appropriate antibiotic. The antibiotic should be performed for at least 14 days, and in case of septicemia for a longer time. Surgical treatment is indicated when there necrotizing cholecystitis and cholelithiasis accompanying vesicular rupture. When a sample of green bile is obtained, treatment should be initiated immediately with antibiotics because bacteria convert the bilirubin into biliverdin (Fossum and Willard, 1997; Oswald et al., 1999).
Ultrasound is an important complementary diagnostic tool for today veterinarian has easy access, so it is of the utmost support for the approach to the diagnosis of cholecystitis, given the specificity of clinical signs and laboratory show .
Patient assessment
In Animal Clinic Hospital of the Faculty of Agriculture and Veterinary one poodle dog, 11 years old he attended.
History
The patient had intermittent vomiting yellow, weight loss, anorexia and urination orange, with an evolution of 15 days. Received diet based on commercial feed and had the vaccination plan and deworming day.
Clinical examination findings
On clinical examination increased temperature (39.8 ° C), great pain during palpation of the cranial abdomen and jaundiced mucous found.
Diagnostic aids
CBC, ALT, AST, ALP, GGT, urea, creatinine, total, free and conjugated bilirubin, cholesterol, albumin, glucose, urinalysis, clotting and liver ultrasound was requested.
Laboratory data showed anemia limit, normochromic normocytic, moderate leukocytosis with neutrophilia, monocytosis and presence of mild signs of cell toxicity ( Table 1 ), increased enzyme activity of ALT, AST, GGT and FAS, increased concentration Total and conjugated bilirubin, decreased glucose and albumin; the values of urea, creatinine and cholesterol were within the reference ranges ( Table 2 ). Urinalysis showed bilirubinuria (++++) ( Table 3 ). The clotting time was 10 minutes.



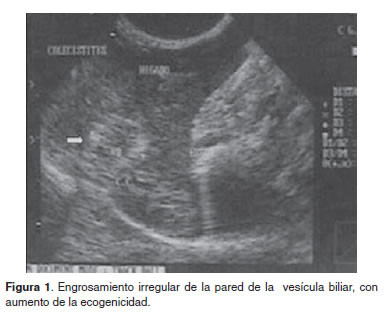
In ultrasonography a gallbladder with thickened walls, thick echogenic content and biliary (bile mud) with presence of particles ranging in size from 3 to 10 mm without acoustic shadowing (observed Figures 1 , 2 and 3 ). The sonographic diagnosis was compatible with cholecystitis.


Treatment approach, evolution monitoring and diagnostics
It was established a treatment based on fluid, antiemetics and antibiotics (amoxicillin metronidazole).
While initially (two days) there was a slight improvement, continuing the clinical picture, it was decided to repeat the blood count and liver ultrasound.
The CBC this time was similar to the first ( Table 1 ), maintaining the anemia, leukocytosis, neutrophilia and monocytosis.
Ultrasound showed with respect to the first a marked increase in liver bile echogenicity and liquid, so it was decided to perform a liver exfoliative cytology by fine needle aspiration, guided by ultrasound.
Cytology said hepatocytes with marked cytoplasmic vacuolization ( Figures 4 and 7 ), cuboidal and columnar low biliary tract ( Figures 5 and 6 ), increased neutrophil and cytolysis karyolysis signs, presence of some lymphocytes and plasma cells ( Figures 5 , 6 , 7 and 8 ). In relation to the cytology results and ultrasound conducting an exploratory laparotomy it was determined, during which cholecystectomy was decided because the wall of the VB was thickened and irregular ( Figure 9 ), and an excisional biopsy of the liver was taken. Histopathology of liver tissue and VB was requested.
For cholecystectomy an incision was made along the midline in the cranial abdomen, he discussed the VB and the visceral peritoneum along the gallbladder and liver influenced union. By blunt dissection he proceeded to release liver and cystic duct to its junction with the bile. To avoid damaging the bile duct, a catheter is placed into the duodenal papilla. It was clamped and made double ligation of the cystic duct and artery. Sectioned duct and gallbladder was removed. Duodenal incision was closed with simple knots of absorbable material and the white line with a simple continuous suture with nonabsorbable monofilament. Subcutaneous tissue synthesis was performed with a continuous suture and the skin with simple stitches, both non-absorbable material.





In pathologic evaluation of postoperative VB, irregular wall thickening, edema and thick, greenish bile, with hard concretions, hard to undo observed, ranging in size from 2 to 8 mm ( Figures 10 , 11 and 12 ).
Histopathological examination revealed lymphocytic infiltration BV in limited foci. In liver tissue lobular maintaining its structure, but with an infiltrate of lymphocytes and neutrophils, some necrotic hepatocytes surrounding marked cholestasis and bile canaliculi thrombus was observed.
The response to medical and surgical treatment was poor and the animal died five days after surgery.




Discussion and conclusions
Given the specificity of clinical signs, in this case suggesting a liver and / or biliary disease, sonographic identification VB abnormalities such as increased wall thickness, presence of biliary sludge and without acoustic shadowing echogenic structures, It was very important at first to recognize the inflammatory disease VB.
The increased values of AST, ALT, FAS, GGT, BT and BC, and hypoalbuminemia bilirubinuria obtained the next day, they were consistent with an obstructive hepatobiliary process, which was not shown by ultrasound in the first study. Hypoglycemia and hypoalbuminemia may be related to the patient's anorexia box. The white blood cell count was consistent with a severe inflammatory and / or infectious condition.
It cytology a chronic inflammatory process indicated by the presence of neutrophils, lymphocytes and macrophages, probably infectious due to the presence of neutrophils with high degree of degeneration; and commitment of the hepatobiliary system due to the presence of altered hepatocytes morphologically and abundant cells of the biliary system. Cytology and histopathology were consistent with a colangiohepatitis.
The first scan showed abnormalities only VB, although results indicated a complementary and hepatobiliary involvement. This may be because a diffuse liver disease, such as cholangitis or colangiohepatitis can have a normal sonographic appearance or diffuse hyperechoic. Clearly, the process began as a condition of BV, then spread to the liver tissue next to it, demonstrated by the second ultrasound and a commitment where that body was observed.
Although all tests were of great diagnostic aid, ultrasound in this case was an excellent tool enabling early diagnosis of vesicular disease. Cholecystitis in the differential diagnosis of those dogs who develop jaundice, abdominal pain, pyrexia and clinical-pathological abnormalities compatible with this disorder should be included.
References
Avgeris S, Hoskinson JJ. Sematosa ENFI cholecystitis. Sel Vet 1996; . 4: 108-109 [ Links ]
Barr F. Diagnostic ultrasound in the dog and cat. Cambridge: Blackwell Scientific Publications; 1992. [ Links ]
Fossum T, Willard M. Diseases of the gallbladder and extrahepatic biliary tree. In: Ettinger S, Feldman E, editors. Treaty of veterinary internal medicine. Diseases of the dog and cat. 4th ed. Buenos Aires: Intermédica; 1997 p.1689-1695. [ Links ]
R Fritsch, M. Gerwing ultrasound dogs and cats. Zaragoza: Acribia, SA; 1996. [ Links ]
Jain N. Essentials of Veterinary Hematology. Philadelphia: Lea & Febiger; 1993. [ Links ]
Kaneko J, Harvey J, Bruss M. Clinical Biochemistry of Domestic Animals. 5th ed. San Diego: Academic Press; 1997. [ Links ]
Loriot N, S Martinot, Franck M. Abdominal ultrasound dog and cat. Barcelona: Masson; 1997. [ Links ]
Nyland TG, Mattoon JS. Co echography diagnosis in small animals. 2nd ed. Barcelona: Ediciones Veterinary Multimédica; 2004. [ Links ]
Oswald PG, Twedt CD, Steyn P. campilobacteriana cholecystitis. Sel Vet 1999; 7: 34-36. [ Links ]
Smith S, D Biller, et al. Imaging of the biliary obstruction. Sel Vet 2001; . 9: 60-67 [ Links ]
Strombeck DR, Guilford WG. Digestive diseases of small animals. 2nd ed. Buenos Aires: Intermédica; 1995. [ Links ]
Share this article / Teilen Sie diesen Artikel