

Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Evaluations of phylogenetic proximity in a group of 67 dogs with
osteosarcoma: a pilot study
Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Canine Periosteal Osteosarcoma
Images added / Abbildungen hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
New subcategory added / Neue Unterkategorie hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
Images added / Abbildungen hinzugefügt 01.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Heart valvular diseases











Contrast-enhanced Ultrasound for Detection of Traumatic Splenic Bleeding in a Canine Model During Hemorrhagic Shock and Resuscitation

Qian Lin, Faqin Lv, Yukun Luo, Qing Song, Qinghua Xu, Yihua Su, Yu Tang, Jie Tang

Background
Contrast-enhanced ultrasound (CEUS) is a highly specific and sensitive method for the detection of abdominal injury. We assessed the value of CEUS for real-time monitoring of splenic trauma and detection of bleeding in a canine model of splenic injury during hemorrhagic shock and resuscitation.
Methods
Forty Grades III and IV traumatic splenic lesions were created in 15 mongrel dogs. Hemorrhagic shock was induced by exsanguination via the left femoral artery. Animals in shock were then resuscitated with 6% hydroxyethyl starch. CEUS was performed continuously to investigate the imaging characteristics of splenic trauma and to monitor changes in bleeding.
Results
Prior to induction of hemorrhagic shock, CEUS revealed active bleeding in 36 of 40 traumatic lesions (90.0%), either as contrast medium extravasation or pooling, both in the spleen and outside the capsule. During the shock period, no traumatic lesion had active bleeding. CEUS revealed that tiny branches of splenic arteries decreased in number and became thinner. The traumatic lesions appeared as nonenhanced areas with poorly defined boundaries. After fluid resuscitation, rebleeding occurred in 30 traumatic lesions, and 28 (93.3%) of these were detectable by CEUS.
Conclusions
CEUS allowed real-time monitoring of splenic trauma and detection of bleeding and rebleeding in hemodynamically unstable dogs, prior to and after fluid resuscitation. This suggests that CEUS might be used in clinical intensive care for patients with traumatic hemorrhagic shock.
Introduction
Methods
Animals
Establishing the animal model
Ultrasound imaging
Results
Creation of an animal model
Comparison of physiological indices among different stages
MAP, SaO2, and splenic length decreased whereas HR increased significantly in all animals with shock. However, MAP, SaO2, and splenic length increased significantly after fluid resuscitation (Table 1).

Perfusion parameters of splenic parenchyma
The parenchymal perfusion parameters, including arrival time, time to peak intensity, peak intensity, and washout time were evaluated (Table 2). During the period of hemorrhagic shock, the arrival time, time to peak intensity, and washout time were significantly longer, and the peak intensity was lower, compared with these parameters prior to shock was induced. Fluid resuscitation significantly reversed all these effects. That is, fluid resuscitation shortened the arrival time, time to peak intensity, and washout time and increased the peak intensity.

CEUS imaging characteristics of splenic trauma
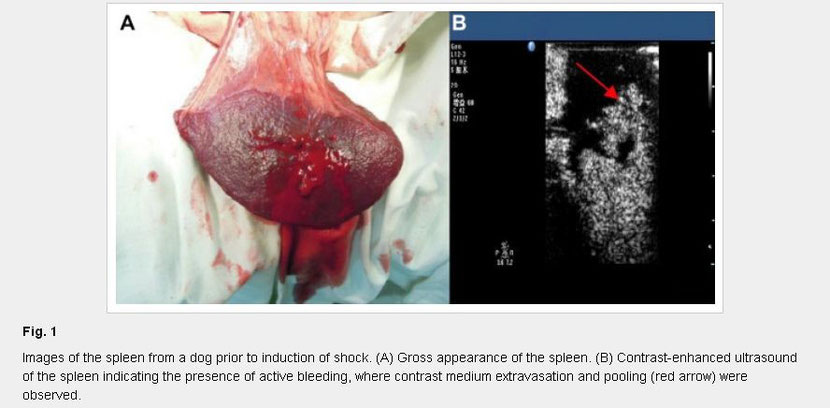
Prior to induction of hemorrhagic shock, the spleen was bright red in color with good elasticity (Fig. 1A). CEUS revealed active bleeding in 36 of 40 traumatic lesions (90.0%), observed as contrast medium extravasation or pooling, both in the spleen and outside the capsule (Fig. 1B).
During the shock period, the spleen significantly shrank and became wrinkled, and had a dark red color and hard texture (Fig. 2A). The traumatic lesions had no visible active bleeding. CEUS revealed that the tiny branches of splenic arteries decreased in number, became thinner, and were dead and branch-like in shape (Fig. 2B). The contrast agent accumulated into floccules at the ends of small arterial branches and was slowly diffused. The traumatic lesions appeared as nonenhanced areas with blurred boundaries, and there were no signs of active bleeding.

After fluid resuscitation, the size of the spleen was similar to that prior to hemorrhagic shock, with a slightly dark red color and recovered elasticity (Fig. 3A). Rebleeding occurred in 30 traumatic lesions. CEUS revealed that the tiny branches of splenic arteries reperfused rapidly. Splenic parenchymal perfusion was enhanced heterogeneously. Twenty-eight of the 30 lesions (93.33%) showed abnormal enhancement, suggesting the occurrence of rebleeding (Fig. 3B).

Discussion
Share this article / Teilen Sie diesen Artikel