

Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Evaluations of phylogenetic proximity in a group of 67 dogs with
osteosarcoma: a pilot study
Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Canine Periosteal Osteosarcoma
Images added / Abbildungen hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
New subcategory added / Neue Unterkategorie hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
Images added / Abbildungen hinzugefügt 01.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Heart valvular diseases











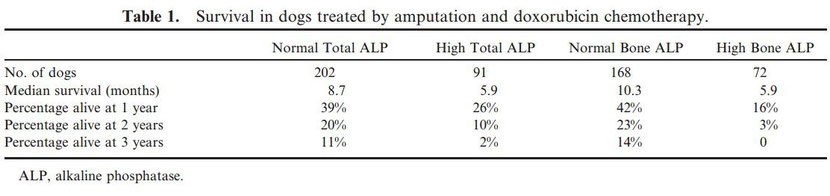
Doxorubicin and BAY 12–9566 for the Treatment of Osteosarcoma in Dogs: A Randomized, Double-Blind, Placebo-Controlled Study

Antony S. Moore, William S. Dernell, Gregory K. Ogilvie, Orna Kristal, Robyn Elmslie, Barbara Kitchell, Steven Susaneck, Robert Rosenthal, Mary K. Klein, Joyce Obradovich, Alfred Legendre, Tara Haddad,
Kevin Hahn, Barbara E. Powers, and Darren Warren,
J Vet Intern Med 2007;21:783–790

Background:
This study was designed to assess the efficacy of a matrix metalloproteinase inhibitor in prolonging
posttreatment survival for dogs with appendicular osteosarcoma after treatment
with amputation and doxorubicinchemotherapy.
Hypothesis:
Survival will be prolonged in dogs receiving BAY 12-9566.
Animals:
The study included 303 dogs with appendicular osteosarcoma.
Methods:
Dogs were treated with doxorubicin (30 mg/m2) every 2 weeks for 5 treatments starting 2 weeks after amputation.
Dogs were randomly allocated to receive a novel nonpeptidic biphenyl inhibitor of matrix metalloproteinases (MMPs, BAY 12-9566; 4-[4-4-(chlorophenyl)phenyl]-4-oxo-2S-(phenylthiomethyl) butanoic
acid) or placebo after doxorubicin chemotherapy.
Results:
Median survival for all 303 dogs was 8 months; and 1-year, 2-year, and 3-year survival rates were 35%, 17%, and
9%, respectively. Treatment with BAY 12-9566 did not influence survival.Multivariate analysis revealed that increasing age (P5.004), increasing weight (P5.006), high serum alkaline phosphatase
(ALP) (P5.012) and high bone ALP (P,.001)
were independently associated with shorter median survival times. Additional analyses on available data indicated that as the number of mitotic figures in the biopsy increased (P5.013), and as
plasma active MMP-2 concentrations increased (P5.027), the risk of dying increased.
Conclusions and Clinical Importance:
Doxorubicin is an effective adjuvant to amputation in prolonging survival for dogswith appendicular osteosarcoma.
Key words:
Angiogenesis; Cancer; Canine; Chemotherapy; Metalloproteinase inhibitor; Metastasis.
Osteosarcoma of the limbs is more common in dogs than in any other species and accounts for more than 80% of malignant bone tumors in dogs. Based on studies of survival after amputation, the
metastatic rate for appendicular osteosarcomas is 98% and the most commonly detected site of metastases is the
lungs.1 Surgical treatment of osteosarcoma by amputation is palliative and increases survival by pain relief, thereby
delaying euthanasia. Survival of dogs with osteosarcoma can be prolonged by adjuvant chemotherapy. Early reports of doxorubicin failed to show efficacy.2
However, larger studies have shown there is a benefit to the use of doxorubicin, given as 5 biweekly doses at a dosage of 30 mg/m.2 In one study, 2 or 3 doses were given before surgery,
and additional doses were given the day after surgery and 2 weeks later. Median
survival was 12 months; 50% of the dogs were alive at 1 year, and 10% were alive at 2 years, thereby approaching a similar
efficacy to that of cisplatin.3 Doxorubicin causes cumulative cardiotoxicity, the risk of which
is higher in breeds predisposed to cardiomyopathy. Many dogs with osteosarcoma also are breeds that are
at risk for cardiomyopathy, and doxorubicin may not be a good choice for these dogs.
Recent studies have revealed that the magnitude of serum total alkaline phosphatase (T-ALP) activity is highly prognostic for dogs undergoing amputation and chemotherapy; dogs with a T-ALP higher
than the upper limit of normal have a worse prognosis than dogs with normal activity regardless of the chemotherapy protocol used. 4–8 Another important prognostic factor identified for dogs with
appendicular osteosarcoma is histologic grade. High grade tumors with histologic evidence of tumor growth into vessels or lymphatics, a high number of mitoses, increased cellular pleomorphism,
small amounts of tumor matrix, and more than 50% necrosis in the tumor biopsy specimen had a worse prognosis compared with low grade tumors. 6
The major characteristics of osteosarcoma are its capacity for invasive local growth and its ability to form metastatic foci at distant sites in the body. Matrix metalloproteinase (MMP) activity
has been implicated in both processes. Matrix metalloproteinases, especially MMP-2 and MMP-9 (gelatinase-B), have been found in a variety of inflammatory and neoplastic conditions of humans, as
well as in various malignancies of dogs. In human patients with osteosarcoma, expression of MMP- 9 in tumor cells that survived neoadjuvant chemotherapy was a stronger predictor of survival than
were either serum ALP activity or percentage tumor necrosis. 9 In more recent studies, expression of MMPs, including MMP-2 and MMP-9, has been associated with a shorter disease-free interval
(DFI). 10 This finding is possibly the result of the enhanced ability of tumor cells expressing MMP-2 and MMP-9 to invade surrounding tissue11 and to metastasize. 12 Canine osteosarcoma biopsy
specimens13 and cell lines14 have been shown to express high concentrations of MMP-2 and MMP-9, and it is likely that these enzymes play a role in the pathogenesis of canine osteosarcoma as
well.
People with cancer who have high MMP concentrations in neoplastic tissues also have increased serum and plasma concentrations of MMPs when compared with normal controls. 15,16 MMPs therefore may
be a unique marker for predicting metastasis. 15 Studies of human patients with lung cancer revealed that the amount of MMP-9 in serum was correlated with poor cumulative survival.
16
Specific inhibitors of MMP activity have been suggested for their potential to increase the metastasisfree period after local therapy (eg, surgery or radiotherapy) and chemotherapy. BAY 12-9566
(4-[4-4-(chlorophenyl)phenyl]-4-oxo-2S-(phenylthiomethyl) butanoic acid) is a novel nonpeptidic biphenyl inhibitor of MMP-2. In addition it has shown inhibitory activity against other MMPs
involved in tumor progression at nanomolar concentrations, specifically MMP-9 and MMP-3 (stromeolysin-1). BAY 12-9566 also has been demonstrated to have efficacy in decreasing tumor regrowth and
the number of metastases in implanted human breast cancer in nude mice. 17 The present study was designed to assess the efficacy of BAY 12-9566 in prolonging survival in dogs with appendicular
osteosarcoma after amputation and doxorubicin chemotherapy.
Materials and Methods
Study Design
The present study was a multicentered, double-blind, placebocontrolled, randomized clinical trial. Adult dogs determined to be in stage IIB osteosarcoma (extracompartmental lesion without
detectable metastasis) were eligible for this trial. Dogs were excluded if they had preexisting evidence of metastases on thoracic radiographs, to regional lymph nodes or to other sites, or if
they had a concurrent disease that required additional therapy or was likely to prevent the dog from living 1 year, or if they had received any chemotherapeutic agents before entering the study.
Before entry, patients were staged by CBC, serum biochemical profile, urinalysis, and thoracic (3 view) and extremity (tumor) radiographs, as well as complete history and physical examination.
From previous literature,3 the estimation for the median DFI of the placebo group was 224 days, and the minimum follow-up time was estimated at 448 days. It was determined that 84 patients (both
treatment groups combined) were needed to detect a 100% improvement in disease-free interval; for a 50% improvement, 187 patients were needed, and 449 patients were needed to detect
a 30% improvement.
Patients
Based on the entry criteria, 312 dogs were entered into the study. Nine dogs were deleted from analysis after entry because they did not meet entry criteria for the following reasons: on
histologic review, 3 dogs had tumors other than osteosarcoma (1 each of hemangiosarcoma, fibrosarcoma, and undifferentiated sarcoma) and 6 dogs had metastases at presentation (3 to lymph nodes
and 3 to lungs). Three hundred and three dogs were entered into statistical analysis for this study. They were analyzed by intent to treat.
Participating sites were Tufts University (95 cases), Colorado State University (95), Veterinary Referral Center of Colorado (32), University of Illinois (16), Greater Houston Veterinary
Specialists (13), Veterinary Specialists of Rochester (13), Southwest Veterinary Specialist Center (11), Animal Cancer and Imaging Center (9), University of Tennessee (9), Fountain Valley (6),
and Gulf Coast Veterinary Oncology (4).
Standard Therapy
Two weeks after amputation, dogs with appendicular osteosarcoma received treatment with doxorubicin (30 mg/m2) every 2 weeks. Doxorubicin was placed in 150 mL of 0.9% NaCl and administered over
approximately 20 minutes through an IV catheter. Treatments were carried out according to the standards set by Good Clinical Practice (VICH GL9)18.
Criteria for delay of treatment included neutropenia ( ,3,000 cells/dL), thrombo-cytopenia ( ,100,000 platelets/dL), or vomiting or anorexia considered to affect quality of life for the patient.
Severe toxicity was defined as sepsis, neutropenia 1 week after doxorubicin ,1,000 cells/dL, or grade 3 to 4 anorexia or vomiting (with standardized forms modified from the Eastern Cooperative
Oncology Group) and resulted in a 25% decrease in doxorubicin dose for the next cycle. If toxicity was not seen at the decreased dosage, the dosage was increased by 10% increments at each of the
remaining doses until a dosage of 30 mg/m2 was achieved. Continued toxicity or the finding of metastatic disease resulted in treatment cessation.
Randomized Trial
BAY 12-9566 was provided for this study by Bayer AG, Leverkusen, Germany, in the form of 200- and 50-mg tablets of the same physical size. In addition to BAY 12-9566, the tablets contained
anhydrous lactose, cellulose, sodium lauryl sulfate, croscarmellose sodium, and magnesium stearate. The placebo tablets were of the same physical size and color; the anhydrous lactate was
increased by the amount of active ingredient removal. Tablets were stored at controlled room temperature.
At entry, dogs were given a unique identification number by a central office. At the fourth doxorubicin treatment, dogs were evaluated by CBC, serum biochemical profile, urinalysis, and thoracic
(3 view) radiographs, as well as a complete history and physical examination. Dogs without clinical evidence of metastatic disease were randomized at this time to receive BAY 12-9566 or placebo.
Assignment was performed by randomization tables at a remote central site, and the coded assignation (letter code) was mailed to the treatment site in a sealed envelope. At the fifth treatment,
final assessment of eligibility was performed (review of staging procedures from treatment 4 and physical examination); if the patient continued on study, the envelope was opened and the
appropriate tablets were dispensed at a dosage of 10 mg/kg body weight (to the closest 12.5 mg [one fourth of a 50-mg tablet]) to achieve dosing accuracy within 10%) to be administered once
daily, with food, by the owner until remission was lost.
Clinicians were blinded as to the identity of the drug used until the final analysis of the study was complete. If metastases were detected, the dog was withdrawn from the study and was allowed
to receive any other therapy that the client and clinician wished. Toxicity was assessed in the same manner as for doxorubicin with standardized forms modified from the Eastern Cooperative
Oncology Group; patients were evaluated every 12 weeks by CBC, serum biochemical profile, urinalysis, and thoracic (3 view) radiographs, as well as a complete history and physical examination to
assess performance (modified Karnovsky) status. At each visit, the remaining tablets were counted, the number recorded, and the next 12-week supply dispensed unless metastatic disease was
identified. Assessment of the number of tablets consumed and the plasma concentrations of drug every 3 months allowed assessment of client compliance in dosing and assured that the correct dose
had been prescribed.
MMP Assay
At each staging visit, blood was collected for MMP analysis at the same time as samples for CBC and serum biochemical profile. A 6-mL heparinized sample was centrifuged within 15 minutes, and
plasma was aliquoted into 2 cryofuge tubes for storage in duplicate at 280uC until further analysis. At the time of amputation, sterile samples of tumor tissue and of adjacent, normal stromal
tissue were collected into separate cryofuge tubes for storage at 280uC. In addition, samples from each site were stored in Z-fix fixative for histopathology. Similar samples were obtained at the
time of disease progression or at postmortem examination.
Tumor and normal stromal tissues were homogenized separately with a mechanical homogenizera with a 3-mm generator in 4 mL cold 50 mM Tris buffered saline, pH 8.0, with 0.25% Triton X-100
detergent. The samples then were centrifuged for 10 minutes at 1500 3 g, and the supernatants harvested and stored at 280uC. Protein content of the homogenized samples was measured by BioRad
detergent compatible (DC) protein assayb (Bradford) with
spectrophotometric measurement performed at 595 nm.
Tissue, stromal, and serum samples were analyzed by gelatin zymography with the NOVEXc system described previously. 19 Briefly, a volume of 10 mg of protein was taken from each homogenate or
serum sample and placed into each well with an equal volume of sample buffer containing 0.5 M Tris-HCl (pH 7.0), 20% glycerol, 4% sodium dodecyl sulfate (SDS, wt/vol), and 0.005% bromophenol
blue. Samples were electrophoresed on a 10% Tris-glycine acrylamide gel, with 0.1% gelatin used as a substrate under nonreducing conditions at 125 V for approximately 110 minutes at room
temperature. The gels then were removed and washed in renaturing buffer (Triton X-100, 2.5% vol/
vol in water) for 30 minutes followed by overnight incubation at 37uC in developing buffer (50 mM Tris, 0.2 M NaCl, 5 mM CaCl2, 0.02% Brij 35 [wt/vol], pH 7.6). Gelatinolytic activity was
visualized by staining the gels with 0.5% (wt/vol) Coumassie blue R250d in 40% ethanol/10% glacial acetic acid solution for 3–6 hours. All gels then were destained in deionized water. Human pro
and active MMP-2 and MMP-9e standards were run on each gel as positive controls.
All of the gels were analyzed wet with a densitometerf by associated software. g To obtain a semiquantitative value for each sample, the optical assessment value of each unknown band was compared
with the optical assessment value of the human MMP standard band (1 ng loaded per gel). A ratio of unknown to
standard then was calculated. An arbitrary unit value was assigned to each patient sample.
Formalin-fixed specimens from tumor and stromal samples were submitted for histopathology and read by 1 pathologist (BEP) to assure that appropriate samples were obtained and to ensure
consistency in tissue grading techniques. Tumor samples were assigned grades of either 1, 2, or 3 based on a cumulative score obtained from histologic examination of criteria including amount of
matrix (1–3; abundant 5 1, moderate 5 2, and scant 5 3),
percentage necrosis (0–3), nuclear pleomorphism (1–3; mild, moderate, or severe), nucleolar size (0–2; small, medium, or large), nucleolar number (0–1; 1 or multiple), and mitosis score (0–4; 0 5
0–10 mitotic figures per 10 high-power fields; 1 5 11–20; 2 5 21–50; 3 5 51–74; 4 5 75 or more). Selection of fields for counting of mitoses was random, avoiding areas of necrosis and abundant
matrix. The total score was added, and tumors with a total score of ,7 were grade 1, 7–9 were grade 2, and .9 were grade 3.
Statistical Analysis
Survival time was chosen as the end point used in this study to facilitate comparison with existing literature. Also, assessment for metastatic disease was done every 12 weeks only until 2 years
after surgery and thereafter as per individual owner and clinician preference, allowing for inconsistency or incomplete data in the measurement of DFI after 2 years (in approximately 40% of the
patients).
The signalment data examined for prognostic significance with regard to survival time were (as categorical variables) sex, neuter status, breed, breed type (working, sporting, herding,
non-sporting, and terrier), location of tumor, bone affected, forelimb versus hindlimb location, and clinic entered from; and (as continuous variables) age and body weight in
kg.
Pathology variables examined for potential prognostic significance were (as categorical variables) amount of matrix (1–3), percentage necrosis (0–3), nuclear pleomorphism (1–3), nucleolar size
(0–2), nucleolar number (0–1), histologic type, mitosis score (0–4), and (as continuous variables) number of mitoses per 10 highpower fields.
Clinical pathology test results examined for potential prognostic significance included (as categorical variables) bivariate evaluation of total ALP activity at entry (high or normal), and bone
ALP activity at entry (high or normal, with normal range 0–45 U/L); and (as continuous variables) serum total ALP activity at entry and serum bone ALP activity at entry.
MMP data examined were tumor and stromal pro and active MMP-2 and MMP-9 concentrations; serum active MMP-2 and MMP-9 concentrations, and plasma active MMP-2 and MMP-9 concentrations. Results of
MMP analysis were categorized as continuous variables by the actual measured concentration, or as a bivariate result (detectable or nondetectable).
Treatment data examined for potential prognostic significance included (as categorical variables) treatment (placebo versus experimental drug) and whether the patient received further
chemotherapy after detection of metastases.
Survival curves for each potential categorical risk factor were created by the Kaplan-Meier product-limit method. Evaluation of potential risk factors on survival time was done by the Cox
forward
conditional regression method. Because values for factors examined in univariate analysis were not available for all dogs, 4 levels of multivariate analysis were performed using those factors
that were significant below the P 5 .05 level on univariate analysis. Histopathology grading was not available for all dogs and was added as a second level of analysis. In addition, bone ALP and
MMP, based on tests that are not commercially available, were separately added into multivariate analysis as a third level after initial analysis. A standard statistical program was used
for
statistical analyses.h
The median age for the 303 dogs was 8 years; there were no dogs 1 year old or less and 5 dogs were 2 years old. The median body weight was 34.2 kg, (range, 8.2–68.4 kg); 14 dogs weighed ,20 kg
and 2 dogs weighed ,10 kg. There were 159 females, 144 males, and 278 were neutered. The most common breed was mixed breed (64 dogs); Rottweilers (50; neutered 5 49, intact 51), Golden Retrievers
(39; neutered 5 33, intact 5 6), and Labrador Retrievers (33; all neutered) were the most common purebred dogs followed by Greyhounds (17), Doberman Pinschers (13), and German Shepherd Dogs (12).
The osteosarcoma affected the forelimb in 196 dogs, and the hindlimb in 107 dogs. The most common site was the proximal humerus (87 dogs), followed by distal radius (77), distal femur (36),
distal tibia (29), and proximal tibia (22); other sites were affected in fewer than 10 dogs each; all but 9 tumors were metaphyseal
(midshaft humerus 5 4; midshaft femur 5 3; midshaft tibia 5 2). Histologic type was available for 225 dogs: the most common was osteoblastic (140 dogs) followed by undifferentiated (34),
fibroblastic (27), and chondroblastic (15); with telangectatic (3), osteoclastic (2), and sclerosing (2) less commonly seen.
Of the 303 dogs entered, 80 dogs developed metastases before randomization. Assessment of client compliance in giving tablets resulted in 11 more dogs that did not receive acceptable dosing of
drug (7 receiving active drug and 4 receiving placebo).
Median survival for all 303 dogs was 8 months; and 1-year, 2-year, and 3-year survival rates were 35%, 17%, and 9%, respectively.
Prognostic Factors
Clinical data were available for all dogs. Serum ALP activity was available for 293 dogs, and bone ALP activity for 240 dogs. Serum total ALP activity was above normal in 92 dogs and within
normal range in 201 dogs; serum bone ALP activity was above normal in 72 dogs and within normal range in 168 dogs. MMP data were available for 213 to 278 dogs depending on the
analysis.
Histopathology scoring data were available for 169 dogs with the exception of percentage necrosis, which was available for 121 dogs; biopsy grade, therefore, was only available for 121 dogs. The
number of mitoses per 10 high-power fields ranged from 5 to 168 (median, 31); 42 dogs had 5–25 mitotic figures, mitosis score 1; 78 dogs had 26–50 mitotic figures, mitosis score 2; 25 dogs had
51–75 mitotic figures, mitosis score 3; and 10 dogs had more than 75 mitotic figures, mitosis score 4.

On univariate analysis, the factors significantly affecting survival were age, weight, ALP (high or normal), number of mitoses, mitosis score, bone ALP, bone ALP (high or normal), serum active
MMP-9 concentration, and plasma active MMP-2 concentration.
Initial multivariate analysis incorporated data for age (P 5 .004), weight (P 5 .006), and ALP (high or normal; P 5 .012), which all retained significance. As age increased so did the risk of
dying; as weight increased, so did the risk of dying. Dogs with high serum ALP had shorter median survival times (Fig 1; Table 1). Because not all dogs had data available for histopathology or
for bone ALP, these were added separately to the multivariate analysis.
When using the subset of dogs for which histopathology data was available (169 dogs), the number of mitotic figures (P 5 .013) and serum ALP (high or normal) retained significance. As the number
of mitotic figures increased, the risk of dying increased.
After removing the histopathology data and adding bone ALP (high or normal; available for 240 dogs), bone ALP (high or normal; P , .001), age, and weight all retained significance. Dogs with high
serum bone ALP had shorter median survival times (Fig 2; Table 1).

When the MMP data (available for 213 dogs) was added to all data other than mitotic figures, bone ALP activity (high or normal), age, plasma active MMP-2 (P5 .027), and weight significantly influenced survival. As MMP-2 concentrations increased in plasma, survival times were shorter (Fig 3).

Factors that did not have a significant effect on survival included treatment (placebo versus active drug), treatment clinic, sex, neuter status, breed, breed type, location of tumor, bone
affected, forelimb versus hindlimb location, ALP activity at entry, cumulative dosage of doxorubicin, histologic type, all other pathology variables listed, all other MMP data, and whether the
patient received additional chemotherapy after detection of metastases.
To further assess the effect on survival of treatment (placebo versus active drug), and to ensure that there was no cryptic group that benefited from the treatment, we selected only the valid
cases for study (212 dogs that had been randomized to receive treatment or placebo after the fifth doxorubicin treatment and were valid as assessed by the measured consumption of drug), and
treatment with placebo versus active drug still had no effect on survival. Also, when we further selected only patients with measurable serum and plasma active MMP-2 or serum and plasma active
MMP-9 concentrations (above 0), there still was no effect of placebo versus active drug.
Cardiomyopathy
Twenty-three dogs were confirmed on cardiac ultrasonography to have decreased contractility, associated with clinical signs of heart disease. The median time to develop cardiomyopathy was 126
days, and ranged from
35 to 1,752 days after entry into the study. Thirteen dogs developed cardiomyopathy ,180 days after entry, and 10 dogs .180 days after entry (Table 2). Eleven of these dogs had metastatic disease
diagnosed concurrently with
cardiomyopathy.
Discussion
This multicentered, randomized clinical trial found that there was no survival benefit to the oral administration of an inhibitor of metalloproteinases 2 and 9 (MMP-2 and MMP-9) in conjunction
with amputation and doxorubicin chemotherapy.
Survival of dogs with osteosarcoma can be prolonged by adjuvant chemotherapy. When evaluating chemotherapy protocols for the treatment of osteosarcoma, median survival times often are very
similar, and the use of 1-, 2-, and 3-year survival rates provides more information as to the likelihood of long-term control and even cure.
In this study, doxorubicin demonstrated efficacy in slowing or prevention of metastasis in dogs with appendicular osteosarcoma with 1-, 2-, and 3-year median survival of 35, 17, and 9%,
respectively. This finding is similar to cisplatin, which has been shown to improve survival rates to a median survival of between 6 and 13 months and 1-year survival rates to between 30 and 62%;
2-year survival rates are between 7 and 21%. 20–24 Carboplatin (300 mg/m2 IV) provides similar survival benefit to cisplatin with a median survival of 10.5 months; 35% of the dogs were alive 1
year after surgery. 8,25 The 2- and 3-year survival rates in the study reported here were higher than those reported in
a previous smaller study of doxorubicin. 3
The disadvantage of doxorubicin therapy compared with the platinum drugs is the risk of doxorubicin cardiotoxicity. In this study, dogs with abnormal cardiac function were not considered eligible
for the study, and breeds considered susceptible to cardiomyopathy were excluded unless echocardiography was considered to be within normal limits. Despite these precautions, nearly half of the
Doberman Pinschers and Great Danes entered developed clinical cardiomyopathy. Although it is not possible to judge whether this rate is higher than for dogs of those breeds not treated with
doxorubicin, the availability of alternative chemotherapy drugs with similar efficacy (carboplatin and
cisplatin) implies that doxorubicin should not be the first choice for adjunctive treatment of osteosarcoma in
dogs of these breeds.

As has been demonstrated in other studies by other chemotherapy protocols, increased serum ALP activity
at presentation (before amputation) is strongly predictive for poor survival after amputation and doxorubicin chemotherapy. A recent study that did not find such an association may not have
included enough patients to make the observation. 26 In addition, high serum bone ALP isoenzyme activity was an even stronger predictor of low long-term survival (1- to 3- year survival rates).
Serum ALP activity may be affected by other disease processes (eg, hyperadrenocorticism) and may not be accurate in individual patients. Unfortunately, bone ALP is not available as a commercial
test; however, these results argue that it could be clinically helpful to be able to obtain such measure-ments. There appears to be value in measuring bone ALP because it may predict dogs that
are unlikely to respond to chemotherapy, allowing either more aggressive treatments to be used or for owners to choose a palliative option.
Tumor grade was not available for all patients despite collection of samples during the study. Some of these specimens were sufficient to make a diagnosis of osteosarcoma (confirming the
diagnosis from laboratories used by each participating institution) but not to provide a subtype. Additionally, some samples were
considered by the pathologist to be inadequate to allow accurate estimation of individual grading criteria (eg,
mitotic rate). Tumor grade itself was not a predictor of survival in this study (with 121 patients); in a previous study of 99 dogs, osteosarcoma grade did predict survival, but the criteria
differed somewhat from those used here (eg, inclusion of vascular invasion). 6 On the other hand, in that study, and in this one, the number of mitoses was a predictor of survival; decreasing
survival times were seen as the mitotic rate increased.
Advancing age was a predictor of poor survival in this study. In a previous evaluation of survival after amputation alone, both younger dogs and older dogs had worse survival rates than dogs between the ages of 7 and 10 years. 1 Although the reasons for the difference are unknown, it is possible that chemotherapy is more effective against micrometastatic disease in younger animals. It is also possible that younger animals had less histologically aggressive tumors. When mitotic rate was added into multivariate analysis, the effect of age was no longer a predictor of survival. Unfortunately, this analysis was only possible for 169 dogs. Age retained significance in all other multivariate analyses.
Increasing body weight also predicted shorter survival in this population of dogs. This effect has been noted previously when carboplatin was used postamputation. 25 In that study, smaller dogs were more likely to live longer, and the suggestion was that chemotherapy dosing by body surface area allows for higher dosing to smaller dogs (ie, smaller dogs presumably have a higher metabolic rate). The same finding in this study argues for increasing chemotherapy dosage in patients that do not show toxicity to chemotherapy at starting dosages. Potentially, increasing doses by 10% for each round of chemotherapy that does not result in clinically relevant acute toxicity could improve survival rates in larger patients.
Finally as plasma active MMP-2 concentrations increased, survival times were shorter. Disappointingly, there was no effect of the study drug, which had been shown to be a potent inhibitor of both
MMP-2 and MMP-9 in preliminary studies. Even when we selected only dogs that were valid as assessed by the measured consumption of drug, or when we further selected only patients with measurable
serum and plasma active MMP-2 or serum and plasma active MMP-9, there still was no effect of placebo versus active drug. It is possible that this drug is not as active in vivo as in vitro, or
drugs may not be effective in inhibition of canine metalloproteinases. It is also possible that treatment with BAY 12-9566 may cause up-regulation of other metalloproteinases in response to
decreases in the target MMPs. This could theoretically offset the benefits of drug therapy. Phase III studies of BAY 12-9566 were discontinued in
human patients with small cell lung cancer after treatment was found to be associated with worse survival at interim analysis. 15
This study was carefully designed as a prospective, randomized, double-blind study. Monitoring by external monitors was performed at regular intervals, and compliance was high. Few patients were lost to study follow-up. For these reasons, the clinical results should be considered as reliable as is currently possible in veterinary medicine.
On the other hand, there were some limitations to this study. At the time this study was conducted, there were no canine-derived standards for MMP-2 and MMP-9; therefore human MMP-2 and MMP-9
standard controls were used. There is considerable sequence homology between MMPs in humans and other species. MMP-2 has 96 to 98% sequence homology among rats, mice, and humans. MMP-9 has 75 to
85% sequence homology among rats, mice, rabbits, humans, and cattle. 27 Therefore, reasonable homology is assumed to exist
between human and canine MMPs. The study analyses were done by gelatin zymography, which is semiquantitative. The enzyme-linked immunosorbent assay (ELISA) and quantitative reverse
transcriptase-polymerase chain reaction (RT-PCR) methods may provide a more sensitive and quantitative evaluation of MMP activity in serum samples. There were no validated methodologies for
canine MMPs at the time of this study.
Acknowledgments
This study was supported by a grant from Bayer Animal Health, Kansas City, MO. The authors acknowledge the help and support of Rodney A. Hansen, PhD, Weber State University, Department of Health
Promotion and Human Performance, Ogden, UT, and Kristi L. Richardson, BS, University of Colorado Health Sciences Center, Denver, CO.
Footnotes
a Mechanical homogenizer, Virtis, Gardiner, NY
b Bradford protein assay, Bio Rad, Hercules, CA
c NOVEX-Invitrogen, Carlsbad, CA
d Coumassie blue R250, Sigma, St Louis, MO
e Human pro and active MMP-2 and MMP-9, CalbiochemOncogene Research Products, Boston, MA
f Densitometer, Molecular Dynamics, Sunnyvale, CA
g ImageQuant, Molecular Dynamics, Sunnyvale, CA
h SPSS 10, Statistical Analytical Software, Chicago, IL
References
1. Spodnick GJ, Berg J, Rand W, et al. Prognosis for dogs with
appendicular osteosarcoma treated by amputation alone: 162 cases
(1978–1988). J Am Vet Med Assoc 1992;200:995–999.
2. Madewell BR, Leighton RL, Theilen GH. Amputation and
doxorubicin for treatment of canine and feline osteogenic sarcoma.
Eur J Cancer 1978;14:287–293.
3. Berg J, Weinstein MJ, Rand WM. Results of surgery and
doxorubicin chemotherapy in dogs with osteosarcoma. J Am Vet
Med Assoc 1995;206:1555–1560.
4. Ehrhart N, Dernell WS, Hoffmann WE, et al. Prognostic
importance of alkaline phosphatase activity in serum from dogs
with appendicular osteosarcoma: 75 cases (1990–1996). J Am Vet
Med Assoc 1998;213:1002–1006.
5. Garzotto CK, Berg J, Hoffmann WE, Rand WM. Prognostic
significance of serum alkaline phosphatase activity in canine
appendicular osteosarcoma. J Vet Intern Med 2000;14:587–
592.
6. Kirpensteijn JK, Kik M, Rutteman GR, Teske E. Prognostic
significance of a new histologic grading system for canine
osteosarcoma. Vet Pathol 2002;39:240–246.
7. Kirpensteijn J, Teske E, Kik M, et al. Lobaplatin as an
adjuvant chemotherapy to surgery in canine appendicular osteosarcoma: A phase II evaluation. Anticancer Res 2002;22:2765–
2770.
8. Vail DM, Kurzman ID, Glawe PC, et al. STEALTH
liposome-encapsulated cisplatin (SPI-77) versus carboplatin as
adjuvant therapy for spontaneously arising osteosarcoma (OSA) in
the dog: A randomized multicenter clinical trial. Cancer Chemother Pharmacol 2002;50:131–136.
9. Foukas AF, Deshmukh NS, Grimer RJ, et al. Stage-IIB
osteosarcomas around the knee: A study of MMP-9 in surviving
tumour cells. J Bone Joint Surg Br 2002;84:706–711.
10. Uchibori M, Nishida Y, Nagasaka T, et al. Increased
expression of membrane-type matrix metalloproteinase-1 is correlated with poor prognosis in patients with osteosarcoma. Int J Oncol
2006;28:33–42.
11. Bjornland K, Flatmark K, Pettersen S, et al. Matrix
metalloproteinases participate in osteosarcoma invasion. J Surg
Res 2005;127:151–156.
12. Ferrari C, Benassi S, Ponticelli F, et al. Role of MMP-9 and
its tissue inhibitor TIMP-1 in human osteosarcoma: Findings in 42
patients followed for 1–16 years. Acta Orthop Scand 2004;75:
487–491.
13. Lana SE, Ogilvie GK, Hansen RA, et al. Identification of
matrix metalloproteinases in canine neoplastic tissue. Am J Vet Res
2000;61:111–114.
14. Loukopoulos P, O’Brien T, Ghoddusi M, et al. Characterisation of three novel canine osteosarcoma cell lines producing
high levels of matrix metalloproteinases. Res Vet Sci 2004;77:131–
141.
15. Zucker S, Cao J, Chen W-T. Critical appraisal of the use of
matrix metalloproteinase inhibitors in cancer treatment. Oncogene
2000;19:6642–6650.
16. Ylisirnio S, Hoyhtya M, Turpeenniemi-Hujanen T. Serum
matrix metalloproteinases-2, -9 and tissue inhibitors of metalloproteinases-1, -2 in lung cancer: TIMP-1 as a prognostic marker.
Anticancer Res 2000;20:1311–1316.
17. Nelson AR, Fingleton B, Rothenberg ML, Matrisian LM.
Matrix metalloproteinases: Biologic activity and clinical implications. J Clin Oncol 2000;18:1135–1149.
18. FDA Good Clinical Practice, VICH GL9. VICH Expert
Working Group. US Department of Health and Human Services
Food and Drug Administrative Center for Veterinary Medicine
(May 9, 2001).
19. Leibman NF, Lana SE, Hansen RA, et al. Identification of
matrix metalloproteinases in canine cutaneous mast cell tumors.
J Vet Intern Med 2000;14:583–586.
20. Shapiro W, Fossum TW, Kitchell BE, et al. Use of cisplatin
for treatment of appendicular osteosarcoma in dogs. J Am Vet
Med Assoc 1988;192:507–511.
21. Straw RC, Withrow SJ, Richter SL, et al. Amputation and
cisplatin for treatment of canine osteosarcoma. J Vet Intern Med
1991;5:205–210.
22. Thompson JP, Feguent MJ. Evaluation of survival time
after limb amputation, with and without subsequent administration of cisplatin, for treatment of appendicular osteosarcoma in
dogs: 30 cases (1979–1990). J Am Vet Med 1992;200:531–533.
23. Kraegel SA, Madewell BR, Simonson E, Gregory CR.
Osteogenic sarcoma and cisplatin chemotherapy in dogs: 16 cases
(1986–1989). J Am Vet Med Assoc 1991;199:1057–1059.
Doxorubicin for Appendicular Osteosarcoma 789
24. Berg RJ, Weinstein MJ, Schelling SH, Rand MW.
Treatment of dogs with osteosarcoma by administration of
cisplatin after amputation or limb-sparing surgery: 22 cases
(1987–1990). J Am Vet Med Assoc 1992;200:2005–2008.
25. Bergman PJ, MacEwen EG, Kurzman ID, et al. Amputation and carboplatin for treatment of dogs with osteosarcoma: 48
cases (1991–1993). J Vet Intern Med 1996;10:76–81.
26. Chun R, Garrett LD, Henry C, et al. Toxicity and efficacy
of cisplatin and doxorubicin combination chemotherapy for the
treatment of canine osteosarcoma. J Am Anim Hosp Assoc
2005;41:382–387.
27. Sang QA, Douglas DA. Computational sequence analysis
of matrix metalloproteinases. J Protein Chem 1996;15:137–
160.
Share this article / Teilen Sie diesen Artikel