
-
Brodey RS, Sauer RM, Medway W. Canine bone neoplasms. J Am Vet Med Assoc. 1963;143:471-95.
-
Misdorp W. Skeletal osteosarcoma. Animal model: canine osteosarcoma. Am J Pathol. 1980;98(1):285-8.
-
Wolke RE, Nielsen SW. Site incidence of canine osteosarcoma. J Small Anim Pract. 1966;7(7):489-92.
-
Salm R, Mayes SE. Retroperitoneal osteosarcoma in a dog. Vet Rec. 1969;85(23):651-3.
-
Lamb C. Bone scintigraphy in small animals. J Am Vet Med Assoc. 1987;191(12):1616.
-
Ostrander EA, Comstock KE. The domestic dog genome. Curr Biol. 2004;14(3):R98-9.
-
Ottaviani G, Jaffe N. The epidemiology of osteosarcoma. Cancer Treat Res. 2009;152:3-13.


Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Evaluations of phylogenetic proximity in a group of 67 dogs with
osteosarcoma: a pilot study
Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Canine Periosteal Osteosarcoma
Images added / Abbildungen hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
New subcategory added / Neue Unterkategorie hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
Images added / Abbildungen hinzugefügt 01.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Heart valvular diseases










A Dog in the Cancer Fight: Comparative Oncology in Osteosarcoma

Alexander L. Lazarides, Allison B. Putterman, William C. Eward and Cindy Eward (2017). "A Dog in the Cancer Fight: Comparative Oncology in Osteosarcoma, Osteosarcoma" - Biology, Behavior and Mechanisms, Associate Prof. Kanya Honoki (Ed.), InTech, DOI: 10.5772/66847. Available from: https://www.intechopen.com/books/osteosarcoma-biology-behavior-and-mechanisms/a-dog-in-the-cancer-fight-comparative-oncology-in-osteosarcoma

Abstract
Since the great Rudolf Virchow advised, “Between animal and human medicine there is no dividing line, nor should there be,” limited attention has been paid to cancer in animals. This is finally changing thanks to a renewed focus on studying pet dogs with cancer. Unlike the laboratory mice who have been the mainstay of animal models of disease, pet dogs share an environment with their human owners, have an intact immune system, and often develop diseases spontaneously in ways that mimic their human counterparts. Osteosarcoma (OSA) – while uncommon in humans - is a common malignancy in dogs. This comparatively high incidence alone renders pet dogs an ideal “model” to conduct translational and clinical research into OSA. Indeed, there are many similarities between the two species with respect to this disease. However, owing to the shorter life span and accelerated disease progression, treatment effects can be assessed much more rapidly in canines than in humans. Overall, dogs represent a unique model to study OSA; this chapter aims to discuss the ways that comparative oncology between dogs and humans are being used from basic science research, to genetics and mechanisms of disease, to tumor biology and finally to developing novel treatments.
Keywords: canine, osteosarcoma, human, comparative oncology, novel treatments, genomic analysis
1. Introduction
Making meaningful advances in osteosarcoma (OSA) therapy has been hindered by the low incidence of the disease in humans. In contrast to the low incidence in humans, OSA is a common malignancy affecting pet dogs. While there are fewer than 1000 new human OSA diagnoses in the USA each year, there no fewer than 10,000 canine cases of OSA every year, by conservative assessments made several decades ago [1, 2]. This relatively high incidence in dogs provides an ideal “model” for conducting translational research and clinical research and for gaining insight into the biology of OSA. This paradigm depends upon canine OSA having specific parallels with human OSA. Indeed, there are many similarities between the two species with respect to this disease: from location of the primary tumors and patterns of metastasis, to the genetic drivers of disease and response to therapy [1]. Because canine OSA is a naturally occurring condition in pets who live alongside us, it arises among the same environmental, dietary and immunologic factors as human OSA. In addition to the similarities, there are several key differences that allow canine OSA to elucidate new information in shorter periods of time. Canine OSA typically displays a more aggressive biology and a much faster rate of metastasis than in humans, with death often occurring within 6 months and with 96% of canine OSA patients dying from the disease [3]. Because of these differences, treatment effects from novel interventions can be seen much more rapidly, with a fraction of the longevity and cost required of human clinical trials. Such comparative, cross-species trials conducted in dogs are often met with enthusiasm by owners and with fewer regulatory hindrances that would face human patients [4]. This field of cross-species cancer research is known as “comparative oncology.” Dogs present to us a unique, powerful and underutilized model to study OSA; this chapter aims to demonstrate and discuss the ways that comparative oncology between dogs and humans with OSA can be used to inform genetics and mechanisms of disease, tumor biology and behavior and the development of novel treatments.
2. Canine osteosarcoma: overview
Osteosarcoma is the most common primary bone tumor in dogs [5–9]. It is estimated to occur in more than 10,000 dogs each year in the USA [1, 10]. This estimate is likely conservative, as the number of pet dogs has increased dramatically since these early studies of the incidence of canine OSA and there are still many dogs who do not receive medical attention. Canine OSA tends to occur in middle-aged to older dogs (median age of 7 years), with a small number of cases presenting between 18 and 24 months of age [11]. Primary rib OSA occurs in younger adult dogs with a mean age of 4.5–5.4 years [12, 13]. Historically, the incidence of OSA in dogs has been considered to be higher in males than females [3, 5–7, 11, 14]; however, more recent data suggest an equal sex distribution [15]. Large and giant breed dogs are predominantly affected. The breeds that are most at risk for OSA are Saint Bernard, Great Dane, Irish setter, Doberman pinscher, Rottweiler, German shepherd and golden retriever. Increased weight and, in particular, height appear to be the most predisposing factors [5–8, 11, 16–19]. Many domestic breeds have narrow genetic diversity due to selective breeding practices, which provides a unique opportunity to more clearly elucidate the hereditary basis of OSA in dogs [15, 20].
Approximately 75% of canine OSA occurs in the appendicular skeleton [6, 13]. Commonly affected sites, in order of frequency, include the distal radius, proximal humerus, distal ulna, distal femur, proximal tibia, distal tibia and diaphyseal ulna [21]. Primary OSA in the axial skeleton has also been well characterized, in order of frequency, in the mandible, maxilla, spine, cranium, ribs, nasal cavity and paranasal sinuses and pelvis [13]. As in humans, OSA of extraskeletal sites is rare but has been reported in the mammary tissue, subcutaneous tissue, spleen, bowel, liver, kidney, testicle, vagina, eye, gastric ligament, synovium, meninges and adrenal gland [22–28].
Dogs with appendicular OSA often present with lameness and swelling at the affected site. There may be a history of mild trauma prior to the onset of lameness and this may cause an acute exacerbation of clinical signs [15, 21]. The signs associated with axial skeletal OSA are site dependent and vary from localized swelling, dysphagia (oral sites), exophthalmos and pain on opening the mouth (caudal mandibular and ocular sites), facial deformity and nasal discharge (sinus and nasal cavity sites) and hyperesthesia with or without neurologic signs (spinal sites) [15]. Dogs with rib OSA often present because of a palpable mass [15].
3. Genetic factors
Development of canine OSA is characterized by the involvement of sporadic and heritable genetic factors. The most thoroughly described gene mutations in dogs are the p53 and phosphatase and tensin homolog (PTEN) tumor suppressor genes and abnormalities in the Rb family members, Rb, p107 and p130. Approximately 60% of canine OSA cell lines overexpress mutant p53 mRNA and protein, which correlates with the presence of missense point mutations within the DNA-binding domain [29]. These findings are corroborated by the identification of mutations in p53 in 41% of spontaneously arisen OSA tumors. The majority of mutations in these cases were point mutations (74%), with a lesser percentage of mutations being deletions (26%). In the absence of a functional p53 protein, its transcriptional target, mdm2, is not present to destabilize the mutant p53 protein and mutant p53 protein accumulates within the cell [30]. Studies have suggested that the RB gene signaling pathway is dysregulated in canine OSA. Analysis of OSA samples identified copy number loss in 29% of cases, resulting in correlative reduction or the absence of RB protein expression in 62% of samples tested [31]. These findings suggest that aberrations in the RB gene likely participate in formation and/or progression of OSA. In addition to p53 and RB gene abnormalities, genomic loss of the phosphatase and tensin homolog (PTEN) tumor suppressor gene is suspected to participate in the genetic pathogenesis of canine OSA. In vitro studies with canine OSA cell lines found that 60% of the cell lines had mutations in PTEN, resulting in the absence of gene transcription and protein translation [29].
4. Diagnostic work-up: local disease
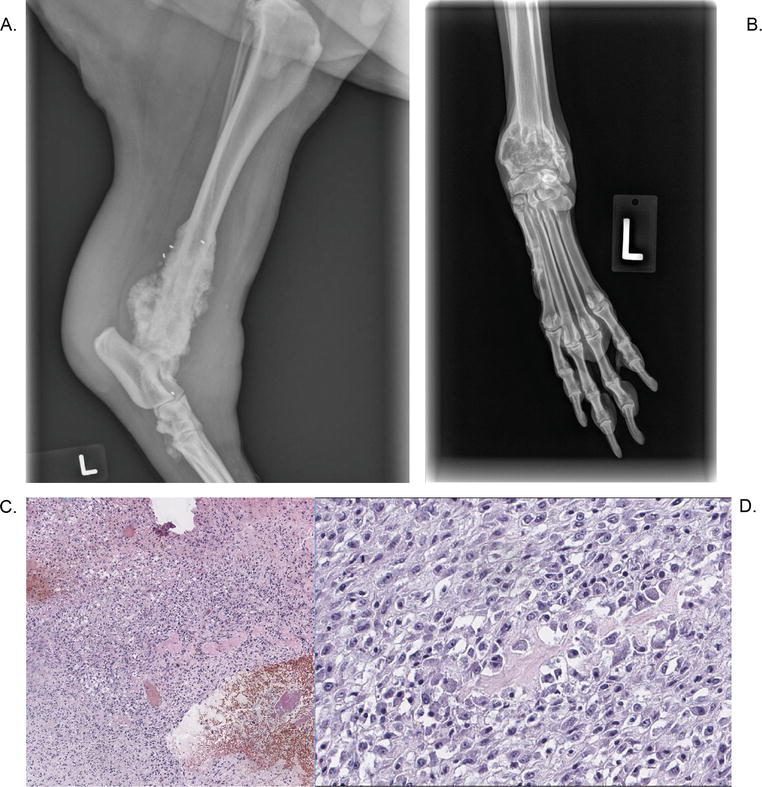
The diagnostic evaluation for dogs with OSA is similar to that employed in humans. Initial evaluation of the primary site involves radiographs. Lesions are typically characterized by a mixed pattern of cortical lysis and periosteal proliferation; however, the appearance of OSA can be quite variable. Commonly observed features include cortical lysis, soft tissue extension with soft tissue swelling and new bone (tumor or reactive) formation. Primary lesions are typically monostotic. Based on signalment (patient-specific factors such as breed, sex, age, etc.), history, physical examination and radiographic findings, a presumptive diagnosis of OSA may be made. Cytology may support a tentative diagnosis. In most cases, a definitive diagnosis is made via histopathology. Bone biopsy is performed prior to pursuing treatment. Samples can be obtained via open incisional, closed-needle, or trephine biopsy techniques. In some cases, repeated biopsy attempts yield “reactive bone,” making it very difficult to obtain the diagnosis preoperatively. Histopathology is performed after tumor removal (amputation or limb sparing) to confirm the preoperative diagnosis. Figure 1 summarizes the elements of the diagnostic work-up of OSA in canines.
Figure 1. Examples of canine osteosarcoma. (A) and (B) Typical radiographic findings including ill-defined lesions with aggressive periosteal reaction and tumor matrix ossification. (C) and (D) High-grade, highly pleomorphic cells with surrounding osteoid.
5. Diagnostic work-up: metastatic disease
Approximately 10% of dogs will have gross evidence of metastatic disease at diagnosis. Fewer than 15% of cases have detectable pulmonary metastasis and less than 8% have metastasis to other musculoskeletal sites. Three view thoracic radiographs are recommended to evaluate for pulmonary metastasis; however, metastases cannot be detected radiographically until the nodules are 6–8 mm in diameter. This underscores the belief that in dogs, as with humans, the presence of metastatic disease on presentation is likely underappreciated. Advanced imaging (e.g., CT, MRI, PET/CT) may be used for patient staging [32, 33]. A thorough orthopedic examination with palpation of long bones and the accessible axial skeleton is necessary to evaluate for sites of bony metastasis. Bone survey radiographs, including lateral views of all bones in the body and a ventrodorsal projection of the pelvis, have been useful in detecting second skeletal sites of OSA [34]. Whereas whole-body bone scans are standard in human medicine, there are conflicting reports on the utility of nuclear scintigraphy for clinical staging of dogs with OSA [35–39]. It can be useful for detection and localization of bone metastasis in dogs presenting for vague lameness or signs of back pain. Although it is a very sensitive imaging modality, it is not specific for identifying skeletal tumors.
6. Prognostic factors
Tumor size, determined as an actual tumor volume or the percentage of bone length affected by tumor, has been found to be a prognostic indicator in dogs. Large tumors have been found to have a poorer prognosis [11, 27, 40, 41]. Tumor location is also a prognostic factor. In general, tumors of the mandible and scapula carry the most favorable prognosis. Other than the mandible and scapula, tumors of the axial skeleton carry a poor prognosis with survival times often less than 6 months. Tumors of the appendicular skeleton are intermediate in prognosis. Specifically, tumors of the appendicular skeleton (radius, ulna, humerus, femur and tibia) are associated with a median survival time of 1 year when treated with aggressive surgery and chemotherapy [21]. Median disease-free intervals (DFIs) and disease- free survival (DFS) times for skull OSA are 191 days and 204 days, respectively. In one study, dogs with mandibular OSA treated with mandibulectomy alone had a 1-year survival rate of 71% [18]. Dogs with maxillary OSA have been found to have a median survival time of 5 months following maxillectomy [42, 43]. A study of orbital OSA reported long-term survival following complete surgical excision [44]. Median survival time for dogs with rib OSA is reported to be 3 months for cases treated with rib resection alone and 8 months for cases treated with resection and adjuvant chemotherapy [45–48]. DFI and median survival time in dogs with scapula OSA was 210 days and 246 days, respectively, with the use of adjuvant chemotherapy increasing DFI and survival time [49]. Survival time of dogs with OSA distal to the antebrachiocarpal (equivalent of human wrist) or tarsocrural joints (human ankle) has a median survival time of 466 days, which is longer than the survival time of dogs with OSA of more common appendicular sites. However, OSA of these sites is aggressive, with a high potential for metastasis [50]. Extraskeletal OSA has an aggressive systemic behavior with a high metastatic rate, with short median survival times ranging from 1 month to 5 months [27, 28].
As in humans, elevated alkaline phosphatase (ALP) has been associated with a poorer prognosis for dogs with appendicular OSA [27, 51–54]. A preoperative elevation of either serum ALP or the bone isoenzyme of ALP (>110 U/L or 23 U/L, respectively) is associated with a shorter disease-free interval and survival. Dogs that have elevated preoperative values that do not return to normal within 40 days following surgical removal of the primary tumor also develop earlier metastasis. At least one study has suggested that tumor grade, characterized by degree of necrosis, mitotic rate and cell differentiation, is also highly prognostic, with higher grade tumors having shorter survival times and disease-free intervals [55].
7. Treatment
Cure is achieved in fewer than 15% of dogs diagnosed with OSA. For the most effective management, multimodality therapy is required to address both local and systemic disease. Amputation, limb-sparing surgeries, as well as nonsurgical techniques, such as stereotactic radiation therapy (SRT), are highly effective for management of local disease (contrary to management of OSA in humans, in which radiation therapy is rarely used). Amputation is the standard local treatment for appendicular OSA and readily allows for adequate surgical margins. It is well tolerated in dogs and offers significant improvement in pain relief and survival relative to palliative treatment. Pelvic tumors are treated with amputation and hemipelvectomy and these patients generally have good levels of function. Rib tumors are treated with thoracic wall resection; mandibular tumors are treated with hemimandibulectomy and maxillary tumors are treated with partial maxillectomy and/or orbitectomy. Limb salvage surgery, most commonly using bone allografts or metal endoprostheses, can be performed in some dogs with appendicular OSA. The most suitable patients for limb salvage are dogs with tumors in the distal radius or ulna [15], but tumors of the scapula, diaphyseal radius and ulna, metacarpus, metatarsus, diaphyseal humerus, femur and tibia and distal tibia have also been treated with limb salvage surgery [21]. Limb function following limb salvage surgery is found to be good to excellent in most dogs and survival is not adversely affected by removing the primary tumor with marginal resection. Intraoperative radiation therapy and extracorporeal intraoperative RT (IORT) have also been utilized in a small number of canine OSA patients. Stereotactic radiation therapy (SRT) is a nonsurgical alternative method which is used on an increasingly common basis for facilitating canine limb salvage. This technique can provide adequate local control of disease in the context of a life expectancy for dogs that is almost always shorter than 2 years, even with systemic therapy.
Although amputation and limb-sparing surgeries, as well as nonsurgical techniques such as SRT, have proved highly effective for management of local disease, the ability to control the progression of OSA metastases remains a clinical challenge. Systemic chemotherapy is the essential component for management of OSA metastases. Protocols that have shown significant improvement in survival include doxorubicin, cisplatin and carboplatin, with medial survival times of approximately 1 year [18, 40, 56, 57]. Lobaplatin has also been used but provides a median survival time of 7 months [21]. No survival advantage has been found when using combination chemotherapy. Despite the aggressive treatment approach, more than 50% of dogs do not live beyond 1 year postamputation and 90% die of disease by 2 years [15]. Further research is needed for discovering effective new combination therapies for improving the long-term prognosis of canine OSA.
8. The dog as a “model” of osteosarcoma
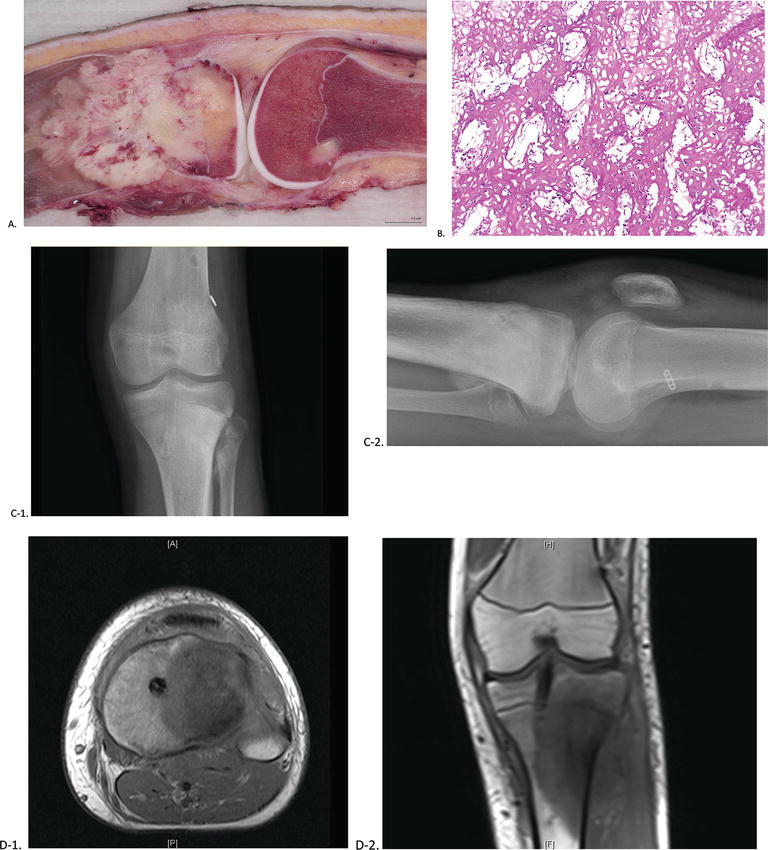
A number of animal models of OSA exist; however, the reliance upon mouse models of OSA has limitations. The canine “model” of spontaneously occurring OSA offers several advantages over non-spontaneous models. It is often described as a “model” (emphasis on quotation marks) because for these patients and their owners; it is not a model at all—they are being treated for a pathologic condition. Naturally occurring OSA in dogs better represents the biological complexity and heterogeneity of the disease than traditional rodent models and, as such, shares a wide variety of epidemiologic and clinical features with human OSA [58]. Genetically, there are far more similarities between dogs and humans than between rodents and humans [59]. Pet dogs share a living environment with humans and are subsequently exposed to many of the same environmental risk factors that contribute to the occurrence of solid tumors in humans. Additionally, tumors in canines occur in the context of intact immune systems, allowing for a better representation of immunologic influence on cancer progression and spread [4]. These tumors are further characterized by high levels of heterogeneity between individuals and between tumors; this heterogeneity is often lacking in traditional models. They also demonstrate the capacity for the development of local recurrence, resistance to treatment and distant metastases, typically to the lungs, just as these tumors do in human patients. Table 1 summarizes the key similarities and differences between human and canine osteosarcoma. Figure 2 summarizes the diagnostic work-up for human osteosarcoma.
Table 1. Comparison of human and canine osteosarcoma

Figure 2. (A) Gross histology demonstrating a destructive osseous lesion with an associated soft tissue mass, (B) high-grade cellular lesion with a trabecular pattern and osteoid production, (C) radiographic findings demonstrating increased sclerosis, with a large periosteal reaction, and (D) MRI images demonstrating cortical destruction and a large soft tissue mass (images collected with permission) [60].
An important power nestled in the study of canine OSA lies in the concept of linkage disequilibrium and the breed structure of canines [61]. Approximately two centuries ago, the practice of selecting canines for certain morphological and behavioral traits grew in popularity, paving the path for modern dog breeds. An unforeseen side effect of breeding was the selection of certain “founder” mutations linked to certain breed-specific traits and diseases. This is seen today in the form of certain breed showing a predilection for species-specific diseases, with the practical result of this “founder” effect being an overall loss of heterogeneity among genes and diseases. Linkage equilibrium is present to a significantly higher degree in canines as compared to humans, making individual breed analysis a strong tool for broad-spectrum genetic mapping [61, 62]. When comparing similar traits between breeds, fine mapping may also be performed, thus making canine models of spontaneously occurring OSA a powerful model for identifying the genetic origins of this disease.
Perhaps, the greatest shortcoming from studying human OSA is the relatively low incidence of the disease. Therapeutics must be evaluated over the course of several years and studies face the challenge of reaching statistically significant power. A solution to this particular challenge is available in the form of cross-species analysis of canine OSA. Canine OSA has an incidence on the order of at least tenfold greater than human OSA [62]. In addition to this significantly larger patient population, dogs also have a shorter life span with faster progression of disease and a shorter period of survival relative to humans [1]. Thus, the collection of data and the evaluation of novel treatments may be carried out more rapidly in dogs than in humans. Although the more rapid life course in dogs is not surprising, as life spans generally decrease along with species size, the reason for poorer outcomes in dogs with OSA is more puzzling. Whether this represents a fundamental difference in treatment (systemic therapy in dogs is relatively less aggressive on a dosage basis) or in disease, biology is not known. Whatever the reason for the difference in survival, the combination of increased patient numbers, time-compressed progression of disease, genetic similarities and spontaneous tumor origin within a natural environmental and immunologic background renders canine OSA an ideal model in which to study the disease.
9. Elucidating the genetic origins of osteosarcoma
The genetic and molecular origins of OSA remain poorly understood. Any given tumor may demonstrate tremendous genetic variation and complexity, characterized by abnormal genetic structural and copy number changes, irregular karyotypes and gross aneuploidy, making elucidation of common pathways more difficult [31, 63, 64]. Dogs with spontaneously occurring OSA present a unique alternative to humans for identifying conserved genetic drivers of OSA. The dog genome was mapped a decade ago and is publicly accessible via the CanFam genome browser, making genetic comparisons with the humans relatively simple [59, 65, 66]. Early genetic studies have demonstrated that canine and human OSAs are virtually indistinguishable. A study by Paoloni et al. used parallel oligonucleotide arrays to compare OSA expression signatures between human and canine samples; interestingly, hierarchical clustering could not segregate the samples by species of origin [67]. Studies such as this demonstrate the tremendous capacity for genomic analysis using comparative oncology; a number of shared molecular targets have been identified using this comparative analysis between canines and humans, including RTK MET, STAT3 and others [68–72].
The breeding of dogs has created artificially selected and refined gene pools. Some breeds of dog, such as Rottweilers and Irish wolfhounds, have also developed a reduced intra-breed genetic diversity and disproportionately higher rates of OSA [17, 73]. This presents an opportunity to examine genetic risk factors for the development of OSA. One study examining the Scottish deerhound used whole-genome mapping to find a linkage for the OSA phenotype. A novel locus was identified on chromosome 34 in a region homologous to human chromosome 3q26, demonstrating a potential genetic basis for the disease in both canines and humans [74]. Another study examined the molecular profiles of dogs with OSA in order to identify subtypes and stratify this disease based on gene expression profiling and its biological behavior. This study was able to identify groupings associated with G2/M transitions and DNA damage checkpoints that correlated with biological activity; additionally, these groupings translated to orthologous human molecular subtypes with similar biological activity [75]. Finally, Angstadt et al. used high-resolution oligonucleotide assays to identify common genome-wide copy number aberrations in both human and canine samples of OSA [76]. Their study reaffirmed a number of known aberrant genes and identified several new genes in regions of instability pointing toward possible players in the genetic origin of OSA. Taken as a whole, these studies demonstrate the capacity for genome-wide analysis and comparisons between dogs and humans to identify possible genetic precursors and drivers of OSA.
Numerous somatic genetic similarities have been identified as a commonality between human and canine OSA, which may help identify new and important insights into OSA biology. p53 and RB1, tumor suppressor genes, are possibly two of the best-known and well-described genetic aberrations in both human and canine OSA. With p53, genetic abnormalities in canine OSA are typically the result of missense mutations, which result in an overexpression of this gene and are present in 41–67% of primary OSA tumors [29, 30, 77]. While p53 is often mutated in primary cases of human OSA, it is found at a much lower rate, with only about 20% of cases showing this abnormality [78]; unlike canine OSA, mutations in the p53 gene in humans are often point mutations [30]. RB1 is a genetic abnormality that is common in human forms of OSA, estimated to be present in 30–75% of cases [79]. While initial studies questioned the putative role of RB1, more recent studies indicate that mutations of this gene are present in 29% of cases of OSA, typically resulting in a reduction or complete absence of the gene product [31, 80]. PTEN is another tumor suppressor gene that has been implicated in both human and canine OSA. Early findings in canine OSA cell lines implicated PTENdeletions and a reduction in gene expression in the development of this cancer [29]; this was confirmed using a comparative genomic hybridization (CGH) genomic analysis in primary canine OSA, which found that PTEN mutations were present in 30–42% of tumors examined [31, 76]. Human studies have similarly identified PTEN as a common mutation present in primary cases of OSA [81].
10. Advances in surgical technique and adjunct therapy
10.1. Surgical and medical therapy for canine osteosarcoma parallels human therapy
There are a number of similarities in systemic therapy and surgical management between human and canine OSA. In both patient populations, en bloc surgical resection, in combination with chemotherapy, is the mainstay of treatment; the addition of either neoadjuvant or adjuvant chemotherapy has further improved survival rates and is now also considered a part of standard of care. Most dogs are treated with adjuvant—rather than neoadjuvant—chemotherapy, as there is less data in dogs regarding the prognostic value of histopathologic response to therapy.
Pioneering of limb-sparing techniques in the surgical treatment of OSA was initially conducted in dogs. One of the early studies of the potential role of limb salvage in canine patients with OSA was conducted by LaRue et al. [82]. This study found that limb salvage in addition to multimodality therapy could represent a viable alternative to amputation in the management of certain patients. A subsequent study by Withrow et al. [83] similarly studied the role of limb salvage surgery as an option in the management of OSA. Forty-nine dogs with limb-sparing resection for OSA of the extremity were followed and stratified by the addition of chemotherapy or chemotherapy with radiation therapy. As in humans, outcomes were significantly linked to percent necrosis, which was improved by a combination of chemotherapy with radiation therapy. Higher rates of tumor necrosis resulted in higher overall survival and better outcomes. The breadth of this data is not as extensive in dogs as it is in humans and the paradigm of chemotherapy/surgery/chemotherapy has not become normative in dogs. Despite similarities in overall survival between amputation and limb-sparing surgery, a significant issue with limb salvage in both canines and humans has been the inadequacy of functional outcomes and the prevalence of postoperative complications. A study by Kuntz et al. [84] examined 17 patients with OSA of the proximal humerus undergoing limb salvage surgery using frozen humeral allografts. As expected, completeness of margins significantly impacted the overall rates of survival, with incomplete margins resulting in an eightfold higher rate of distant metastases. As in humans, when comparing limb salvage with amputation, there was no statistically significant difference in overall survival. However, postoperative functional outcomes and rates of complications were deemed to be unacceptable. Only 12% of patients had good or excellent outcomes with many of the dogs treated with limb salvage suffering from biomechanical failure of their mechanical constructs and 41% of patients receiving limb salvage surgery required conversion to amputation. A retrospective study of human OSA by Rougraff et al. found limb salvage demonstrated similar outcomes with respect to disease-free survival and overall survival when local control via limb salvage is compared to local control via amputation [85]. This has similarly been borne out in canine OSA [18].
The addition of chemotherapy to the management of OSA has dramatically improved outcomes and become a mainstay of treatment for both dogs and humans with OSA. The overall survival of dogs treated with amputation is significantly improved by the addition of chemotherapy. In addition to the previously mentioned studies conducted by LaRue et al. and Withrow et al. [82, 83], 30 dogs with appendicular OSA were evaluated in a study evaluating overall survival rates when treated with and without the addition of cisplatin [86]. Mean survival time was 190 days for patients treated with amputation alone; mean survival time improved to 315 days with the addition of cisplatin. Similar results were found in a study by Berg et al. [56], which examined 22 dogs with appendicular OSA treated with surgical resection with and without the addition of cisplatin. They found a statistically significant increase in survival with the addition cisplatin to surgical management. Interestingly, there was no survival difference between chemotherapy in addition to amputation and limb-sparing surgery, though the cohort numbers were likely too low to draw significant results in this regard. Thesis parallels in the medical and surgical management of OSA across species contribute to canine OSA being particularly well suited in comparison with humans undergoing similar treatment [87–89].
10.2. Novel therapeutics and immunotherapies
Canine models have been an important avenue by which to examine novel therapeutic strategies for OSA. With the advent of intra-arterial chemotherapy, randomized control trials were conducted in dogs with spontaneously occurring OSA to evaluate the safety, efficacy and feasibility of this method of delivery in the treatment of OSA [82]. With the advent of intra-arterial chemotherapy, randomized control trials were conducted in canines with spontaneously occurring OSA to evaluate the safety, efficacy and feasibility of this method of delivery in the treatment of OSA [83]. Similarly, dose escalation studies conducted in canines with OSA have allowed for optimization of chemotherapeutic drug delivery in humans. In a study by Paoloni et al., a phase I dose-escalation study was conducted with rapamycin delivery in canines with the simultaneous collection of multiple pre- and posttreatment biopsies and whole blood sampling to establish efficacy and ideal drug pharmacokinetic time points, data that would have been more challenging to collect in human patients [90]. These insights were translated into a human clinical trial of rapamycin, allowing for a better understanding of dosing and efficacy of the drug [91, 92]. These studies allowed optimization of the dose and delivery of chemotherapy in humans with OSA while allowing for earlier screening of treatments that may have a less than favorable therapeutic index before being tested in humans [93, 94]. Beyond cytotoxicity and optimization studies, canines with OSA have also served as the ideal models for identifying and evaluating novel therapeutics.
Early insights into the role of the immune system in OSA disease progression came about by happenstance while studying canine OSA. While studying outcomes in canines undergoing the combination of limb salvage and chemotherapy, Lascelles et al. found that postoperative infection significantly improved survival [95]. These findings were also recapitulated in humans, as a study by Jeys et al. demonstrated; humans with deep infection following limb salvage for OSA experienced a 35% increase in overall survival rate [96, 97]. These survival benefits were hypothesized to be related to an upregulation in the natural antitumoral activity of the host immune system. This has inspired new investigations into the specific role of the immune system in OSA and the ways in which cancer suppresses the natural immune response. Analysis of canines with and without OSA has identified myeloid-derived suppressor cells (MDSCs) and regulatory T cells (Tregs) that may play a role in suppression of the natural antitumor response of the host [98, 99]. These cells normally function to prevent the antitumoral response from overaction and resultant autoimmunity. Suppressing these cells has been hypothesized as a means of promoting the antitumoral response to improve outcomes in OSA. Although some have associated increased ratios of Tregs with poorer outcomes in canine OSA [100], there remain questions as to whether Treg levels are actually different from healthy controls [99]. MDSCs have also been found to be overrepresented in canine OSA, as demonstrated in two studies by Sherger et al. and Goulart et al. [101, 102]. Similar to Tregs, the role of MDSCs in OSA remains unclear, though increased monocyte counts have been associated with worse outcomes and decreased rates of DFS [103, 104]. Despite the ambiguity surrounding their potential role in OSA progression, Tregs and MDSCs highlight the potential for immune targets in the treatment of OSA.
Immunotherapy for sarcoma is an exciting new field of cancer treatment currently being investigated in both humans and canines. One such agent, liposomal muramyl tripeptide phosphatidylethanolamine (L-MTP-PE), had its first success demonstrated in dogs with spontaneously occurring OSA. This synthetic molecule is an analog of a bacterial cell wall component and a potent activator of monocytes/macrophages. It can be incorporated into liposomes and has been shown to selectively induce monocytes to kill tumor cells [105]. In a study of 40 dogs receiving standard therapy with surgery and cisplatin, canines were randomized to receive the addition of either L-MTP-PE or a placebo. Patients receiving L-MTP-PE had significantly better rates of overall survival as compared to placebo [106]. This study has translated to human pediatric patients with OSA as well, with results indicating L-MTP-PE as a possible adjunct in the repertoire of treatments available for OSA [107, 108].
While immunotherapy is an exciting realm of novel therapeutics in canines with OSA, the canine model is equally beneficial in evaluating the safety and efficacy of a variety of novel therapeutics and novel applications of existing therapies [109]. One such application is the use of aerosolized delivery of chemotherapeutics for pulmonary metastases, which has made significant progress thanks to research conducted in dogs with OSA. A translational study by Rodriguez et al. examined the effect of aerosol delivery of gemcitabine to pulmonary metastasis in dogs with OSA [110]. This study demonstrated an increased in Fas expression and increased rates of apoptosis in pulmonary metastases. Cross-species drug development using canines as a model for human OSA has also been suggested for targets including genetic abnormalities (TP53 and murine double minute-2), growth factors (c-MET and mTOR), angiogenesis (VEGF and HIF-1a) and metastasis (membrane-type-1 matrix metalloproteinase) [23, 54, 90, 111–116].
11. Conclusion: challenges and limitations
OSA remains a challenging diagnosis with little change in the prognosis for several decades. Recognizing the utility of studying animals with diseases shared by humans, Rudolf Virchow stated in the mid-nineteenth century, “Between animal and human medicine there is no dividing line, nor should there be.” Yet despite a desperate need to investigate OSA in greater numbers and scope, dogs with naturally occurring OSA were not seriously studied until the late twentieth century. Man’s best friend provides us an opportunity to study one of our most dreaded diagnoses in larger numbers than we could ever hope to study in humans alone. With similar disease features and treatment algorithms, research may be carried out in dogs in a more facile manner than in humans. Continuing to expand our understanding and awareness of canine, OSA will be a critical step in developing novel and better therapeutic strategies.
Several challenges do remain [93]. While canine models show an accelerated disease progression as compared to humans, this timeline is still significantly longer than murine models. While funding for mouse models of cancer is widespread, funding for the investigation of canine cancer remains sparse. Some novel therapies, such as species-specific antibodies and proteins, may not translate from canines to humans and vice versa. Finally, regulatory oversight and ethical care mandate that some study designs are simply not feasible in pets. Despite these limitations, this review demonstrates that canines are an ideal—and underutilized—model to deepen our understanding of osteosarcoma and to translate exciting developments from the laboratory into the clinic.
Share this article / Teilen Sie diesen Artikel