

Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Evaluations of phylogenetic proximity in a group of 67 dogs with
osteosarcoma: a pilot study
Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Canine Periosteal Osteosarcoma
Images added / Abbildungen hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
New subcategory added / Neue Unterkategorie hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
Images added / Abbildungen hinzugefügt 01.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Heart valvular diseases











Tube Cystostomy VS Bladder Marsupialization: Clinical and Ultrasonographic Evaluation in Dogs

Gaber E, El-Khamary A, Abdelwahed RE. Tube Cystostomy VS Bladder Marsupialization: Clinical and Ultrasonographic Evaluation in Dogs. www.scopemed.org/?mno=162716 [Access: December 09, 2016]. doi:10.5455/ajvs.162716

Abstract
The objective of current study was to evaluate outcomes and complications following tube
cystostomy and bladder marsupialization, as emergent techniques for urine diversion in case
of urine retention. An experimental study conducted on 12 mongrel breed male dogs. Urine
retention was induced by experimental urethral obstruction through ligation of the penile
urethra. Short term follow-up was taken through which clinical and ultrasonographical
examination were carried out. Tube cystostomy and bladder marsupialization were conducted
as a solution (6 cases for each). Outcomes and complications within 14 days postoperatively
were recorded for both techniques. Both surgical techniques were associated with
considerable postoperative complications. Tube cystostomy proved advantageous although
higher cost. It cleared less morbidity than bladder marsupialization. Clinical findings revealed
urine scalds in different degrees in all dogs treated with bladder marsupialization and one
showed mucosal prolapse followed by death. While, hematuria and accidental dislodgement
were the only complications observed in tube cystostomy treated dogs and were easily
managed, except one dog died 2 days after surgery with unknown cause. Ultrasonographic
findings revealed minimal reversible changes of bladder contour with mild cystitis in dogs
treated by tube cystostomy rather massive irreversible changes with severe cystitis and
fibrosis in bladder marsupialization treated dogs. Surgical tube cystostomy is more effective
emergent solution for complete urethral obstruction in dogs than bladder
marsupialization.Using of tube cystostomy is a preferred procedure even it costs more in dogs
kept indoors for longer periods with the need for maintaining urinary continence and
subsequent owner compliance.
1. INTRODUCTION
Acute complete obstructive urolithiasis is a potentially life threatening affection in dogs. It remains a difficult problem to treat and choose one surgical technique in preference to another and
depends on many factors. Acute urine
diversion in case of complete urethral obstruction is an essential to relieve the urine retention and save the life of the animal (Fortier et al., 2004 and Ewoldt et al., 2006). Along the
previous years, many techniques were developed
to deal with that problem. Each one has its own advantages and disadvantages, which in turn, raise the need for developing and modifying new techniques to overcome those complications. Surgical
treatment of urine retention due to urethral obstruction was expanded to include both short and long-term procedures in dogs. Success rate varied and depend on several factors. Starting from
urethrotomy, urethrostomy and cystotomy with urethral retrograde hydropropulsion, and passing by bladder marsupialization, surgical tube cystostomy and minimal invasive surgical tube cystostomy
with their short and long-term complications, ending with the low profile cystostomy tube, the obstructive urolithiasis could be overcome. Tube cystostomy for urinary diversion was initially
described in 1965 as a treatment for ruptured bladders in steers (Hastings, 1965). Since then, it has become popular as a treatment for
obstructive urolithiasis in many species of animals especially in small ruminants(Rakestraw et al., 1995). In dogs and cats, tube cystostomy and bladder marsupialization was trialed to manage the
urethral disorders especially urethral calculi or obstruction to determine the possible outcomes associated with both techniques (Barsanti et al., 1985; Dhein and Person, 1989 and Williams and
White, 1992). Tube cystostomy provides an alternative for urethrostomy and urethrotomy that have poor long-term outcomes (Haven, 1996). Diversion of urine via tube cystostomy is occasionally
performed in small animals but reports of its clinical use are limited in dogs and cats (Hayashi and Hardie, 2003 and Beck et al., 2007).Tube cystostomy is indicated in the temporary and
permanent urine diversion (Williams and White, 1992). Indications for temporary urine diversion includes; acute bladder or urethral trauma,
surgical repair of the urethra, and urinary obstruction (Cornell, 2000 and Beck et al., 2007). Urethral healing occurs after the tube is placed so the animal began to urinate through the normal
urine course rather than the tube. Long-term tube cystostomy is indicated in neurogenic bladder atony or transitional cell carcinoma. Although tube placement has no effect on survival times, all
owners reported that the tube was easily managed at home (Cornell,
2000; Hayashi and Hardie, 2003 and Pearce et al., 2003). Urinary bladder marsupialization was developed in an attempt to provide long-term resolution for urinary obstruction in small ruminants
not intended for slaughter. Although originally developed as a final recourse when other procedures had failed, Bladder marsupialization has been moderately successful in restoring urination in
goats (May et al., 1998 and Ewoldt et al., 2006). It does eliminate
urinary continence and may, as a result, be unaccepted to some owners (Ewoldt et al., 2006).It had an improved long-term outcome when compared with other surgical procedures or when financial
considerations dictated
selection of a more economical procedure.Urinary bladder marsupialization in dogs was reported to be associated with extensive urine scalding problems, stomal stricture and bladder mucosal
prolapse through the fistula site, significant risk of ascending urinary tract infection and loss of urinary continence, cystitis and peristomal skin dermatitis, all rendering the procedure
unacceptable for house hold dogs (Dhein and Person, 1989; May et al., 2002;
Fortier at al., 2004 and Ewoldt et al., 2006).Abdominal ultrasound of the urinary tract is very helpful in diagnosis of urinary tract affections (James at al., 1976 and Espada et al., 2006). It
provides excellent anatomical
information and provides accurate data as sensitivity 90%; specificity 98% and accuracy 97% (Heitz et al., 1980; Malave et al., 1980 and Webb et al., 2000). Ultrasound is characterized by easy
imaging using a suitable probe,
providing adequate sensitivity, specificity, evaluating and following up urine retention process after complete urethral obstruction (Widmer at al., 2004). Present investigation designed to
evaluate which of bladder marsupialization and surgical tube cystostomy could be a reliable alternative technique.
2. MATERIALS AND METHODS
Twelve apparently healthy, adult, sexually intact, mixed breed dogs, having body weights of 12 to 31 kg and age of 3-10 years were selected after subjection to physical examination to assess
their fitness and then prepared routinely
for aseptic surgery. All procedures were performed at the Department of Surgery, Faculty of Veterinary Medicine, Damanhour University. They received 8.75 mg/kg body weight of potentiated
amoxicillin-calvulanate antibiotic
(Synulox RTU 175 mg/ml. Pfizer, Italy) injected intramuscularly one day before operation and extended for 3 successive days post-operatively. All dogs were premedicated with Xylazine HCl and
Atropine sulphate. General anesthesia was induced and maintained with Ketamine HCl. Experimental urethral obstruction was performed by ligating the penile urethra around its course at the ventral
surface of the os-penis. The os-penis was pushed cranially from its caudal origin then a urinary catheter was introduced from the external urethral orifice to obtain a demarcated urethra (Fig.1).
A suture material was passed around the urethra in a circumferential manner using silk No. 2 and tightened to obtain a secured and complete urethral obstruction. After the dogs were being
experimentally suffered from complete urethral obstruction, they were subjected to clinical and ultrasonographical examination. Urine diversion using two different surgical corrective procedures
was carried out for management of
urine retention; bladder marsupialization (6 dogs) and tube cystotomy (6 dogs) was conducted.
Fig (1): Pushing of the os-penis and inserting a urethral catheter

Bladder marsupialization: Little evacuation of the bladder by needle aspiration was carried out after bladder exposure following laparotomy. When the bladder was found ruptured,
the urine in the abdomen was aspirated by suction irrigation and the abdomen was lavaged using slight warm saline. The apex of the bladder was identified and exteriorized using gentle traction
and stay sutures were placed at each end of the intended cystotomy site at the ventral surface of the bladder using suture needle with non absorbable suture material (silk 2/0). An approximately
3 cm cystotomy wound was made in the ventral surface near to the ventral abdominal wall. Urine and sediment was
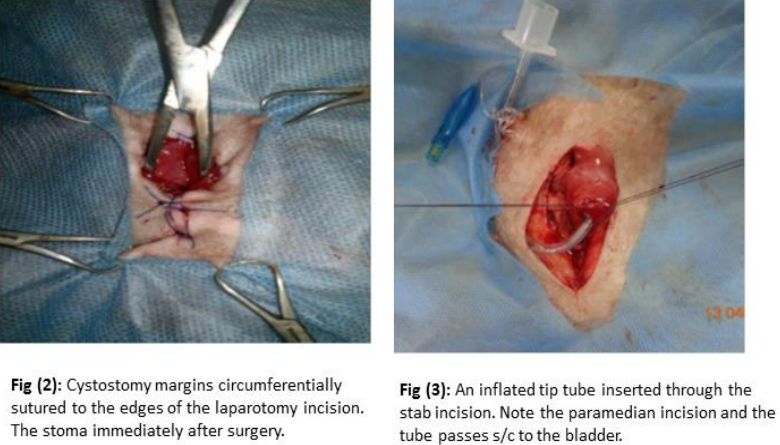
removed by aspiration and lavaged with warm sterile saline solution. The cystotomy margins were then circumferentially incorporated into the caudal aspect of the laparotomy incision during its
closure by suture to the skin (Fig. 2). Care was taken to ensure that bowel was not entrapped by the bladder. The rest of the celiotomy wound was closed in a routine pattern.
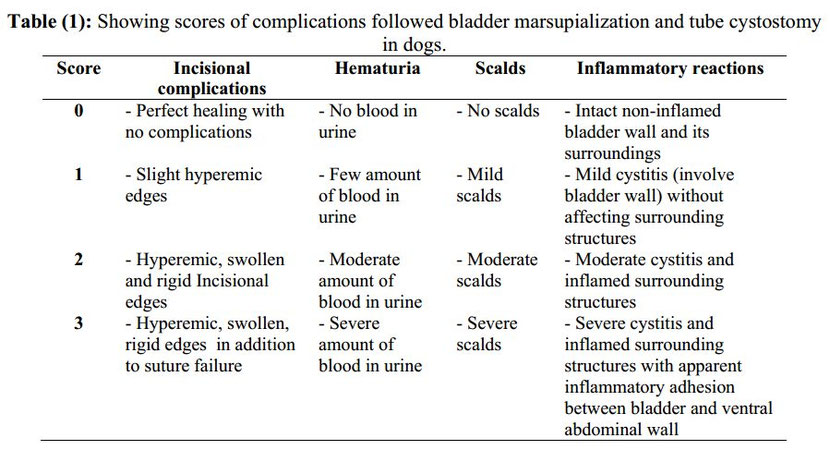
Tube cystostomy: After laparotomy, the bladder was adequately exteriorized and isolated by laparotomy sponges. Purse-string suture was placed in the ventral surface of the bladder using 2/0 silk. Small paramedian incision through the body wall 2-5 cm distance from the ventral midline incision was done. Stab incision at the center of the purse-string suture in the bladder wall was done. A tube is passed through the paramedian incision and into the bladder lumen through the stab incision then the tube tip was inflated with air to prevent the tube from getting out the bladder incision (Fig.3). Bladder was then rested into the abdominal cavity and the ventral midline incision was routinely closed and the tube was anchored to the skin using non-absorbable suture material (silk No.1). Evaluation of both corrective techniques was carried out by clinical and ultrasonographical examination depending on; operative time (time elapsed from incision to skin closure, in minutes), number of incisions, cost, intra and postoperative complications including; incisional complications, hematuria, scalds, inflammatory reactions and stomal characters. Some of the previous parameters were illustrated in number of scores (Table.1). The collected data is subjected to statistical analysis using SAS (2004).
3. RESULTS
Clinical Findings:
Urethral ligation was effective and induced acute complete urine retention between 2-3 days that was reflected negatively on the health condition of the animal. Deterioration of the general
health condition indicated by in-appetence, depression and abdominal colic. The colic was manifested by starting to turn behind in a circle, looking, licking, biting and sometimes kicking the
skin area over the bladder and os-penis.
Intra operative findings:
During exploratory celiotomy for corrective surgery, bladder appeared with severe enlargement and congested wall, severe reddish discoloration mixed with bluish patches covered bladder wall, and
the superficial blood vessels running over the bladder wall was very clear and congested (Fig.6). Bladder marsupialization required one abdominal incision, proved effective, less cost and safe
corrective method (Table.2).Animal showed normal urination from
the new pass way directly at the same day of operation indicated by continuous moistened area around the bladder skin opening. The length of the final bladder stoma to the abdominal wall varied
from 3 to 6 cm.Tube cystostomy required two incisions, proved efficient and useful technique for experimental urethral obstruction. There was no significant difference for operative time between
marsupialization and tube cystotomy (Table. 2).
Postoperative clinical findings:
Tables (3 & 4) showed the postoperative clinical findings following bladder marsupialization and tube cystotomy.
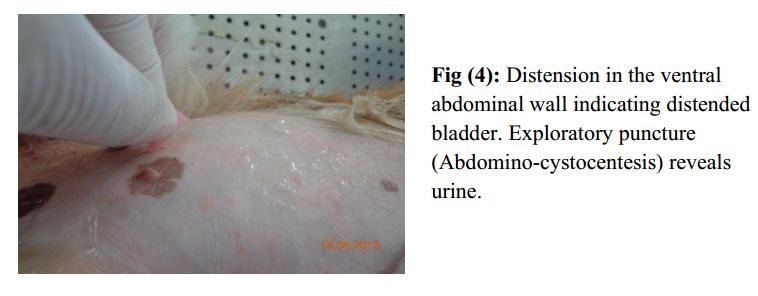
A clinically distended bladder was indicated by distension in the ventral abdominal wall. Abdomino-cystocentesis revealed urine (Fig.4).
Ultrasonographical findings :
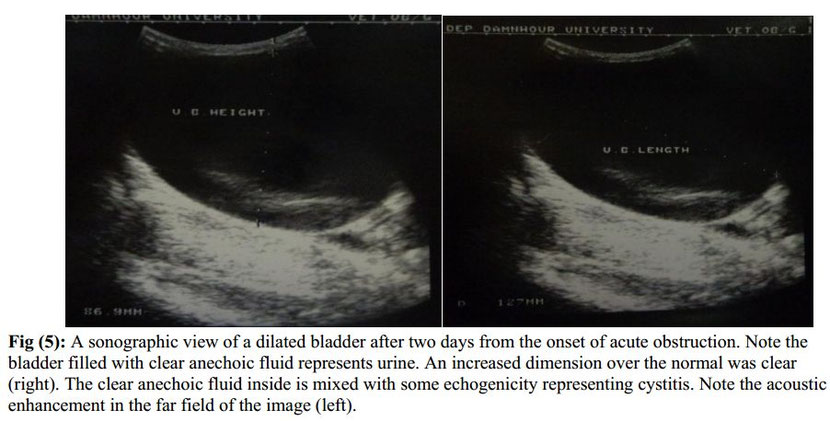
After two days from acute urethral obstruction, enlarged and stretched bladder filled with anechoic substance was evident. Dimensions of the distended bladder were 85-88 mm transversely; 98-104
mm diameter and 125-130
mm longitudinally from cranial to caudal (Fig.5).
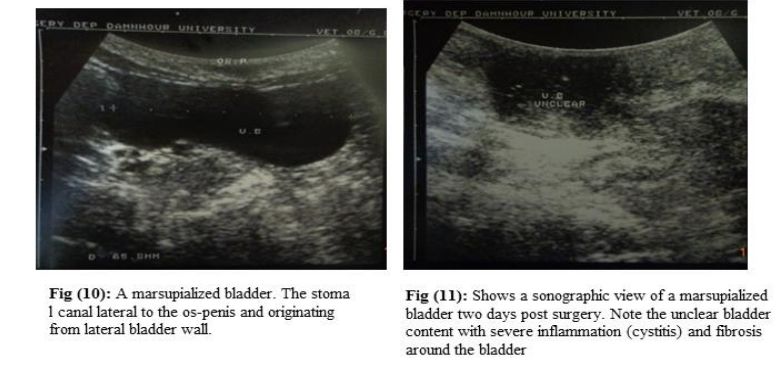
Three days post operation, the permanent stomal wall of bladder marsupialization treated dogs appeared slightly hyperemic and swollen. Slight narrowing and mild scald were observed and the skin surrounding the stoma was moistened with blood tinged urine (Fig.7).
Ten days post operation, the stoma appeared with slight rigid wall, continuous urine flow, and mild scald noticed in skin of ventral region close to the bladder and its stoma (Fig. 8).The ventral
aspect of the os-penis appeared moistened with urine. One case underwent acute urethral obstruction followed by corrective bladder marsupialization was found dead after two days and the bladder
was found everted outside the body with necrotic appearance (Fig.10). In one case underwent tube cystotomy, there was a bloody plug seen inside the tube inhibited
passage of urine partially, directly after the operation. Another case was found dead after 2 days with no apparent tube.




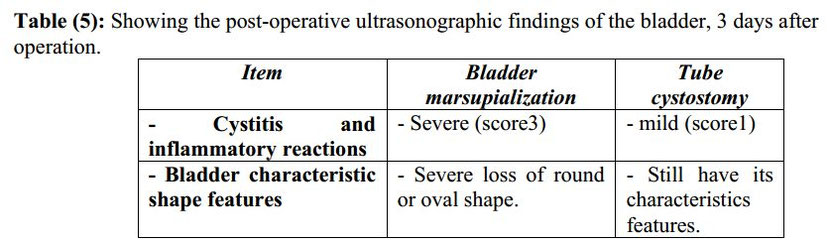
Ultrasonographical postoperative findings (Table. 5):
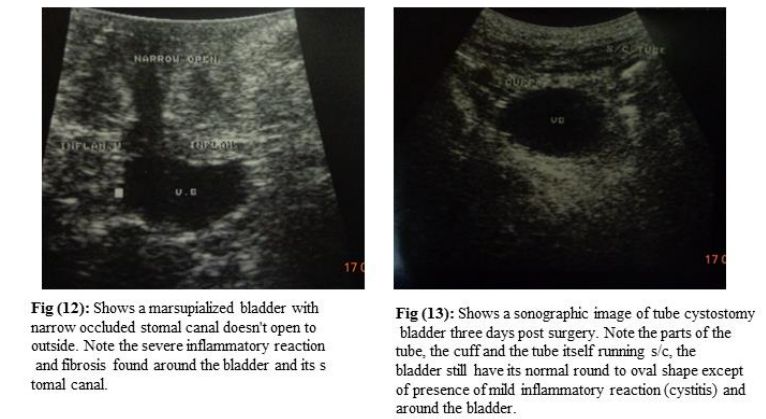
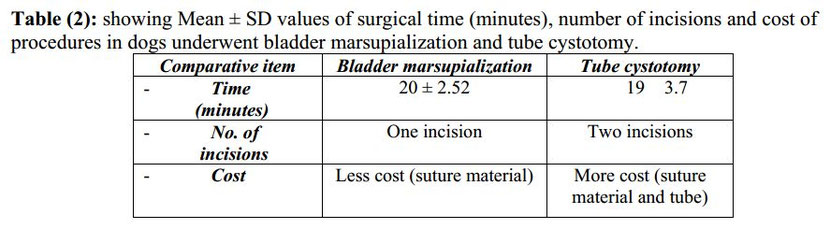
Clear anechoic content and unobstructed canal to the surface of skin at the side of Os-penis were identified by ultrasound indicating normal marsupialized bladder (Fig.10). Cystitis and
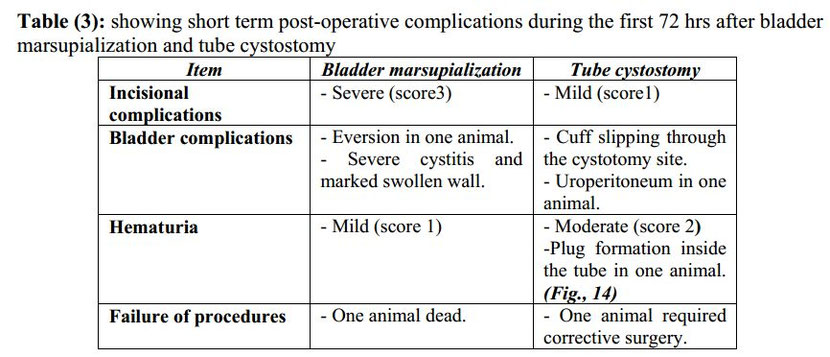
inflammatory reactions proved severe (score 3) following bladder marsupialization (Figs.11 & 12) rather mild (score 1) following tube cystostomy (Fig.13).Bladder characteristic shape features
showed severe loss of round or oval shape in cases subjected to marsupialization (Fig. 11 & 12) rather cases of tube cystotomy those still have its characteristics features (Fig. 13).


3. DISCUSSION
This study proved that bladder marsupialization provided an easily, valid option with only one procedure technique, that doesn't necessitate a 2nd surgical corrective intervention. Similar
findings were observed by (May et al., 1998 and
May et al., 2002). On the contrary, this technique is considered of limited success due to high morbidity rates as a result of extensive urine scalds, stomal stricture and bladder mucosal
prolapse in addition to the severe cystitis and loss of bladder contour and urethral function forever with poor prognosis for breeding and loss of urinary continence (May et al., 1998; May et
al., 2002 and Ewoldt et al., 2008). Although no significant difference was found between the two techniques, marsupializing bladder outside to the skin consumes time required to tube securing
inside the bladder and fixing the tube to the skin.
Enhanced inflammatory reaction was evident after 3 days to take apart in the quick fibrosis and peristomal skin dermatitis. This confirmed the previous experiences of May et al., (1998); May et
al., (2002) and Fortier et al., (2004) who used an absorbable suture material. Stomal stricture and complete occlusion was fastened in the present study coincided with (Ewoldt et al.,2006 and
Ewoldt et al., 2008)and could be attributed to minimum stomal care, severe
peristomal skin urine scalds, dermatitis and severe cystitis. May et al., (2002) showed that complete stomal occlusion happened at day 150 of operation, while in the present study, it happened at
day 21 of marsupialization and it is
considered one of the major drawbacks of bladder marsupialization (Fortier et al., 2004 and Ewoldt et al., 2008).
During this study, one dog was found dead after two days with a prolapsed bladder mucosa. May et al., 1998) treated such complication by mucosal resection. Mucosal prolapse may be attributed to oversized abdominal fascial incision. The mean of dog stomal cystotomy and fascial incision that didn't lead to mucosal prolapse is ranging from 2-3cm maximally according to the body weight. Those lengths were previously supported by Hurwitz and Ehrlich, (1983). The cause of death is unknown and it couldn't be attributed to the bladder mucosal prolapse.
In this study,bladder marsupialization was performed by single incision technique. May et al., (1998) and May et al., (2002) reported that single incision technique could potentially result in
increased severity of urine scalds, while
Ewoldt et al., 2008) preferred the single incision technique. Herein, this technique was hypothesized and proved to lessen the urine scalds due to the slight paramedian position to the prepuce.
Gravity dependent urine descends
from the bladder stoma helped not to cover wider and wider area of the peristomal skin and subsequently, less urine odor and more owner compliance. That is in the contrary to double incision
technique with craniolateral paramedian
position of bladder stoma that led to urine contaminated wide area of peristomal skin. Inthe available two reports conducted by May et al., (1998) and May et al., (2002) in which double incision
technique was preferred, where
low number of complications are reported, statistical comparison of the single and double incision techniques wasn't made. Therefore, a further study is suggested to be performed comparing the
two different techniques of bladder marsupialization.
Cystostomy tube placement had no effect on the survival rate of dogs if it wasn't associated with tube accidental dislodgement (Cornell, 2000 and Beck et al., 2007) In the contrary, in the
currentstudy, one animal was found dead after few days of tube cystostomy placement. Fortier et al., (2004) reported mortality percent in surgical tube cystostomy more than bladder
marsupialization. Examination revealed disappearance of the tube and closure of the
stoma and these findings suggested accidental dislodgement. The cause of death may be attributed to urine leakage, Uroperitoneum, peritonitis and uremia. Ewoldt et al., (2006) confirmed these
findings and added that the most
common cause of death shortly following the tube cystostomy placement is urine leakage.Failure of tube cystostomy in two cases of the study under investigation is attributed to tube displacement
and blockage of the tubes by urine
sludge or blood plug enhanced by hematuria.Fortier et al., (2004) described the catheter obstruction as a common and serious complication requiring careful management to avoid the need for repeat
surgery. Ewoldt et al., (2006) suggested using Foley catheter to be of wide diameter to reduce the incidence of reobstruction. In the current experiment, retrograde flushing of the tube with
saline was efficient and quick managemental solution especially through the first two days post surgery in which hematuria was evident.
In the current study, no free abdominal fluids or minute amount was relevant concurrent with acute urethral obstruction with extreme bladder distention, suggesting that intra-abdominal fluids, if present, is mainly due to urine leakage from the cystotomy site and insecure tube placement inside the bladder. A similar clarification was raised by Hayashi and Hardie, (2003). Ewoldt et al., (2006) believed that extreme bladder distension allowed microscopic
holes developed within the bladder wall leading to urine leakage intraabdominally.
Hematuria, as a minor complication demonstrated in both procedures specially the first two days after surgery, is not a high interpretive complication in bladder marsupialization, while in tube cystostomy, hematuria fastens the formation of urine sludge or the bloody plug and their subsequent tube obstruction (Fortier et al., 2004 and Beck et al., 2007).
Tube cystostomy had mild Incisionalcomplications if compared to bladder marsupialization which had the highest grade of incisional complications (extensive cystitis, urine scalds, stoma occlusion and mucosal prolapse) as described previously by (Fortier et al., 2004 and Ewoldt et al., 2008). The direct contact between the irritant urine and skin in marsupialization is the main factor, while, in the tube cystostomy, was lessened too much as urine pass from bladder to outside environment through tube.
The severely stretched bladder wall, concurrently with change of the color, made the bladder wall very sensitive and difficult to manage during evacuation process for cystostomy incision and
subsequent tube insertion and its securing with purse string suture. Once the severely stretched wall was approached, even by a needle, an irregular and
involuntary increased opening was formed. This enhanced, by way or another, the incidence of urine leakage resulted from irregularity of the cystostomy incision and insecure tube placement and
this could be a reasonable explanation for intraabdominal fluids. Ewoldt et al., (2006) reported that bladder color wasn't predictive of outcome and some animals with red-purple bladders at
surgery recovered well. Depending on this study results, bladder color could be
predictive of the degree and duration of bladder distention. So, it could be predictive of surgery outcome.
Ultrasonographic examination of the bladder
marsupialization 3 days post-surgery revealed marked change in the gross appearance of the bladder. This may be attributed to the severe cystitis, increased fibrosis around the bladder and at
bladder skin interface and accumulation of large amount of exudates inside the bladder. All that confirmed that it was nearly impossible that a marsupialized bladder could return to its normal
function after a certain period. Those manifestations are similar to those described by Cohen et al. (1978) and May et al., (2002) and might subsequently predispose the quick stomal
stricture and occlusion. This proved that ultrasonography is a successful tool not only for diagnosis of urinary tract obstruction but also for the follow-up the process and post operative
examination. Follow-up after tube cystostomy
revealed a bladder still maintain its characteristic features and shape with mild inflammatory reaction (cystitis) which suppose that bladder underwent tube cystostomy placement could return to
normal function easily after tube
removal and maintaining the urethral function again. Also the tube, itself, could be assessed inside the bladder and subcutaneously. An inflated cuff appears sonographically and indicates the
integrity of the tube cuff and subsequent secure placement of the tube inside the bladder. The tube lumen, running subcutaneously, could be checked for presence of any obstruction or tearing in
s/c part. Any adhesions or fibrotic reactions in both techniques could be seen and identified ultrasonographically.
Owner should be aware that marsupialization lead to loss of urethral patency and subsequently the normal urination (through urethra) and the breeding ability will be lost forever. In the
contrary, tube cystostomy preserves the urethral
integrity for both urination and breeding. So, surgical tube cystostomy is considered the most successful surgical treatment for obstructive urolithiasis in small animals including dogs and cats
and this is in agree with what previously
mentioned by (Williams and White, 1992; Fortier et al., 2004 and Ewoldt et al., 2008). The major drawback of surgical tube cystostomy is the cost associated with the procedure, because animals
must be hospitalized during the waiting
period before catheter occlusion coinciding with Fortier et al., (2004) and Ewoldt et al., (2008). Bladder marsupialization is typically a single procedure technique and therefore might be less
costly than tube cystostomy which may need a second corrective interventional procedure with more hospitalization days and more costs. Tube
dislodgement followed by corrective intervention (reinsertion of the tube, or inserting another tube or converting to another surgical procedure as marsupialization makes additional costs
coinciding with Fortier et al., (2004) and Ewoldt et al., (2008). It is therefore possible to conclude that use of tube cystostomy is a preferred procedure even it costs more in dogs kept indoors
for longer periods with the need for maintaining urinary continence and subsequent
owner compliance.
4. REFERENCES
Ewoldt, J.M., Anderson, D.E., Miesner, M.D.,
Saville, W.J. 2006. short and long-term outcomes
and factors predicting survival after surgical tube
cystostomy after treatment of obstructive
urolithiasis in small ruminants. Vet. surg. 35 (6):
417-422.
Fortier, L.A., Gregg AJ; Erb, H.N., Fubini, S.L. 2004.
Caprine obstructive urolithiasis: requirement for 2nd
surgical intervention and mortality after
percutaneous tube cystostomy, surgical tube
cystostomy, or urinary bladder marsupialization.
Vet. surg. 33 (7): 661-667.
Hastings, D.H. 1965. Retention catheters for
treatment of steers with ruptured bladder.
J.Am.Vet.Med.Assoc. 147: 1329-1330
Rakestraw, P.C., Fubini, S.L., Gilbert, R.O., et al.
1995. Tube cystostomy for treatment of obstructive
urolithiasis in small ruminants. Vet. Surg. 24:498-
505.
Dhein, C.R., Person, M.W. 1989. Prebubic or
suprapubic catheterization of eight dogs with lower
urinary tract disorders. J.Am.Anim.Hosp.Assoc. 25:
272-276
Williams, J.M., White, R.A.S. 1992. Tube
cystostomy in the dog and cat.
J.Small.Anim.Practice. (32): 598-602
Barsanti, J.A., Blue, J., Edmunds, J. 1985. Urinary
tract infection due to indwelling bladder catheters in
dogs and cats. J.Am.Vet.Med.Association. (187):
384-388
Haven, M.L. 1996. Comments on tube cystostomy in
small ruminants. Veterinary Surgery. (25): 351-352.
May, K.A., Moll, H.D., Wallace, L.M., Pleasant,
R.S., Howard, R.D. 1998. Urinary bladder
marsupialization for treatment of obstructive
urolithiasis in male goats. Vet. surg. 27 (5): 583-
588.
May, K.A., Moll, H.D., Duncan, R.B., et al. 2002.
Experimental evaluation of urinary bladder
marsupialization in male goats. Vet. Surg.
(31):251-258
Pearce SG; Dearo AC; Howard BE and Brisson BA
(2003): '' management of obstructive urolithiasis
and concurrent urethral rupture in a goat '', Aust.
Vet. J., 81 (5): 268-270.
Cornell KK (2000): '' cystotomy, partial cystectomy
and tube cystostomy '', clinical techniques in small
anim. Pract., 15 (1): 11-16.
Hayashi, K., Hardie, R.J. 2003. Use of cystostomy
tubes in small animals. Compend.
Contin.Educ.Pract.Vet. (25): 928-934.
Beck, A.L., Grierson, J.M., Ogden, D.M., Hamilton,
M.H., Lipscomb, V.J. 2007. Outcome of and
complications associated with tube cystostomy in
dogs and cats: 76 cases (1995-2006). Journal of
Am. Vet. Med. Associat. 230 (8): 1184-1192.
James, A.E., Osterman, F.O., Bush, R.M. 1976. The
use of compound B-mode ultrasound in abdominal
disease of animals. Vet Radiology. (17):106-111.
Espada, Y., Novellas, R., Gopegui, R.R. 2006. Renal
ultrasound in dogs and cats. Vet. Res.
communications. 30 (5): 133-137.
Webb, J.a.w. 2000. Ultrasonography and Doppler
studies in the diagnosis of renal obstruction. BJU
Int. 86 (8): 25-32.
Heitz, F., Carlier, B., Guinet, P., legrand, J.J., Viard,
P.F. 1980. Exploration echtomographique du rein
normal et pathologique du chien et du chat. Rec
Med. Vet. (9):156-363.
Malave, S.R., Neiman, H.L., Spies, S.M., Cisternino,
S.J., Adamo, G. 1980. Diagnosis of hydronephrosis:
comparison of radionuclide scanning and
sonography. AJR. 135 (7): 1179-1185.
Widmer, W.R., Biller, D.S., Adams, L.G. 2004.
Ultrasonography of the urinary tract in small
animals. J. Am. Vet. Med. Associat. 225 (1): 46.
21. Cote, E., Carrol, M.C., Beck, K.A., Good, L.,
Gannon, K. 2002. Diagnosis of urinary bladder
rupture using ultrasound contrast cystography: in
vitro model and two case-history reports. Vet. Rad.
Ultrasound. 43 (3): 281-286.
Hurwitz, R.S., Ehrlich, R.M. 1983. Complications of
cutaneous vesicostomy in children. UrolClin North.
Am. (10):503-508.
Ewoldt, J.M., Jones, M.L., Miesner, M.D. 2008.
Surgery of Obstructive Urolithiasis in Ruminants.
Vet. Clin. Food Animal. (24): 455-465.
Steerer, R.N., Washburn, K.E., McCauley, C.T.,
2002. Percutaneous tube cystostomy and vesicular
irrigation for treatment of obstructive urolithiasis in
a goat. JAVMA. (221):546-549.
Share this article / Teilen Sie diesen Artikel