

Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Evaluations of phylogenetic proximity in a group of 67 dogs with
osteosarcoma: a pilot study
Article added / Artikel hinzugefügt 01.10.2021
Generally Articles and Discussions about Osteosarcoma in Dogs
→ Canine Periosteal Osteosarcoma
Images added / Abbildungen hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
New subcategory added / Neue Unterkategorie hinzugefügt 02.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Pulmonary vessels
Images added / Abbildungen hinzugefügt 01.05.2019
Generally Sonography Atlas of Dogs →
Cardiovascular system → Heart valvular diseases











The Treatment of Malignant Tumours of Bone in the Dog by Intra-Arterial Injection or Perfusion of Epodyl (Triethyleneglycol Diglycidyl Ether)*

Owen, L. N. “The Treatment of Malignant Tumours of Bone in the Dog by Intra-Arterial Injection or Perfusion of Epodyl (Triethyleneglycol Diglycidyl Ether).” British Journal of Cancer 18.2 (1964): 407–418. Print.

OSTEOSARCOMIA is the most common tumour of bone in the dog
although chondrosarcoma, fibrosarcoma, haemangiosarcoma and other less common primary or metastatic
tumours of bone also occur. Brodey, Saver and Medway (1963) found that of 50,750 dogs examined between 1952 and 1962 at the University of
Pennsylvania Hospital, 152 had bone sarcomas
whereas during this same period only 2 dogs with benign bone
tumours were observed.
iod only 2
dogs with benign bone tumours were observed.
Osteosarcoma is
more common in the large breeds and it appears
that the Great
Dane and St. Bernard have the greatest predisposition. The origin is
common in the
distal radius, proximal humerus and distal tibia but rare in the distal humerus and
proximal radius. Tumours occur in other long and in flat bones.
There is considerable variation in the speed of growth. Some
rapidly growing vascular tumours can destroy a large area of bone in 3 weeks whereas other
denser, more
cartilaginous tumours may develop
over a period of
months.
Amputation of the affected limb in large breeds is rarely
performed in Great Britain and no records
of survival are available. A large dog has difficulty in
balancing after the removal of a forelimb, and often shows
over-extension of the opposite carpus. The development of lung metastases is usually rapid
so that
euthanasia rather than amputation is recommended. Brodey, Saver and Medway (1963) have described the results of amputations carried out in Pennsylvania
on 21 dogs.
Most dogs did not
die naturally but were killed in the terminal stages of the
disease with metastases in the lungs and
frequently in other sites. Following amputation
10 dogs were dead
within 3 months and a further 8 died between 3 and 7
months. Only
3 dogs lived for
longer than 10 months.
Knight (1963, personal communication) has treated a small number of
cases of
osteosarcoma by
X-irradiation and while some remarkable histological changes were observed there
were no cures and
the development of lung metastases was not prevented.
Silver (1964), who treated osteosarcomas by
X-irradiation or the intra-arterial injection
of tritiated " Synkavit " obtained disappointing results. Even in cases where there
was relief of
pain and reduction in tumour size there was recurrence
or metastasis
necessitating the destruction of the dog.
The treatment of spontaneous
tumours in dogs
with cytotoxic drugs has been attempted by McCoy, Allison, Crossley and Wannermacher (1956) using
MEPA (3-(oxapentamethylene)N'N" diethylene
phosphoramide), by Irfan (1958) using chlorambucil and by Owen (1962) using the tumour-inhibiting epoxide
Epodyl (triethylene glycol diglycidyl ether). Regional perfusion of cytotoxic drugs in normal dogs has been described by Ryan (1960) and by Boyland, Staunton and Williams (1961). Owen
and Stevenson
(1961) treated a
dog with
bilateral osteosarcoma of the radius by limb perfusion using nitrogen mustard in the extracorporeal circulation.
In a recent recorded series
of osteosarcomas in man high dosage supervoltage radiotherapy was used at 2 MeV delivered by means of
large fields which extended well beyond the radiological and clinical boundaries of the tumour. Surgical
ablation where necessary was postponed for a year. Twelve patients out of 48 were alive and free from disease 5 years later (Westminster Hospital, 1960). It is thus not justified at the present time to attempt chemotherapy for this condition unless radiotherapy fails.
Usually the blood supply to the tumour area has been severely damaged by irradiation and consequently
attempts at the treatment of osteosarcomas in man by perfusion techniques have not often been attempted.
Apart from the more rapid growth of osteosarcomas in the dog in comparison with man, the conditions are similar and attempts to destroy the tumour in the dog by drugs should give an indication of what may happen in man.
METHODS
Administration of Epodyl
Three methods of
administering Epodyl were used: intra-arterial injection, injection into the anterior half of the body
with occlusion of the aorta and by perfusion of a limb.
Intra-arterial injections.-As Epodyl is an alkylating agent and
extremely toxic if applied locally to tissues, percutaneous injections were not attempted. A small incision was made above the stifle or elbow joints, the femoral or brachial arteries were exposed and Epodyl was injected directly into them. When repeated injections were given a fine polythene catheter was inserted via a branch into the main artery and securely ligated in position. The catheter was sealed and left full of heparin saline between
injections.
Usually the
drug was injected
diluted with twice its volume of water in about half a minute. Rapid
injection was avoided as experimentally it was found that this produced severe oedema of the
limb.
In one dog a slow intra-arterial drip of the drug in very dilute solution was given, by suspending the diluted drug about 10 feet above the dog to overcome systolic blood
pressure.
The occlusion of the aorta.-Tumours of the proximal humerus
or ribs are impossible to perfuse for anatomical reasons. In an attempt to localise the drug
in the anterior half of the body and so obtain a higher concentration of drug in contact with the tumour and at the same time to protect the kidneys and the pelvic bone marrow, the aorta was occluded at the level of the last
rib.
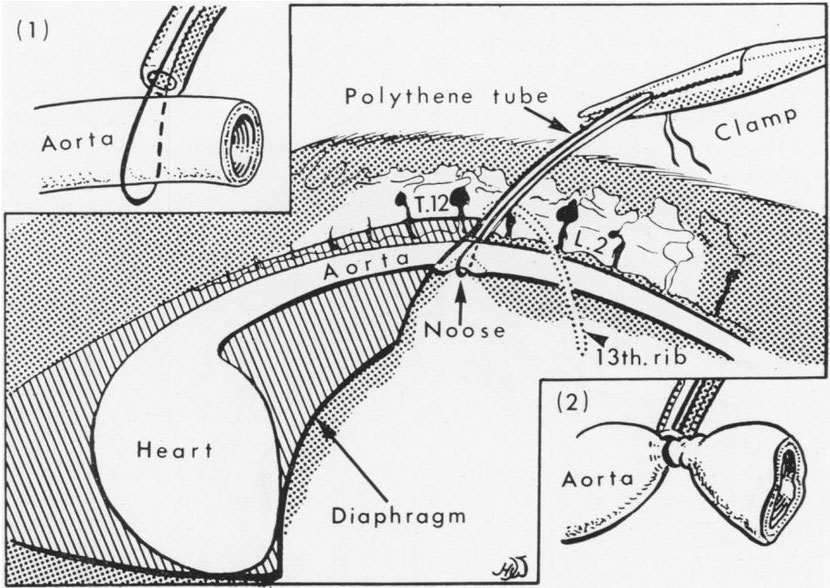
The last rib on
the left side was removed from its periosteal bed and an incision made at this site produced a
small split in
the upper posterior pillar of the diaphragm which exposed the aorta cranially to the coeliac
artery. Braided nylon (30 lb.) was passed around the aorta and threaded through polythene tubing
(size 4) so that a snare was formed around the
aorta.
The polythene tubing was guided posteriorly through the muscles at the operation site and exteriorised through a small skin incision about 3 cm. posterior to the upper edge of
the main incision. The diaphragm was sutured and the original incision closed in the usual way. Occlusion of the aorta was effected by puffing on the braided nylon and applying a pair of artery forceps to
the nylon adjacent to the polythene tubing to maintain a tight snare around the
vessel (Fig. 1). When the femoral pulse could no longer be detected diluted Epodyl was injected into a
vein or artery in the anterior half of the body and allowed to
circulate for ten minutes.
With the dog tilted head downwards at an angle of 45 degrees the tourniquet on the aorta was then slowly released. The downward position and slow release prevented shock occurring.
FIG. 1.-Diagram
showing the site and method of occluding the
aorta.
Between injections the external end of the polythene tubing and emerging nylon strands were left covered with adhesive tape to prevent entrance of air and a resultant pneumothorax. At the
completion of treatment (2-6 injections) some of the external polythene tubing was cut away exposing clean nylon and this nylon was then completely removed by puffing on one end. During the time
the snare remained in the dog daily injections of one mega of penicillin were given.
Perfusion.-The apparatus used has been previously described (Owen and
Stevenson, 1961)
and was essentially similar to that described by Creech, Krementz, Ryan and Winblad
(1958).
Anaesthesia was induced with thiopentone and maintained with nitrous oxide, oxygen and halothane. Occasionally other anaesthetics were used.
Following exposure of the median vessels above the elbow or the femoral vessels about the
region of the mid-shaft of the femur, any small adjacent branches were ligated and the fascia adherent to the main artery and vein were stripped.
Heparin (2.5 mg./kg. bodyweight) was injected intravenously into the dog and after applying bulldog
clips the exposed vessels were incised horizontally. Tapered nylon cannulae were firmly tied in both
artery and vein, a wider bore cannula being used
for the vein. A tourniquet of rubber pressure-tubing threaded through a flanged metal tube (Fig. 2) was applied as high as possible to the limb and clamped
with strong forceps.
FIG. 2. The type of tourniquet used during perfusion of the limbs.

The extra-corporeal circulation consisting of 1200-1300 ml. of cross-matched heparinised fresh canine
blood at a
temperature of 410 C. was then connected to the limb and, depending on
the size
of the dog, about 100 mg. papaverine was
injected into
the arterial system to produce vasodilation of the limb vessels. The flow rate of the perfused blood varied with the size of the dog and ranged from 70-240 ml./min. The diluted Epodyl was divided into approximately 3 equal doses and injected at
10 minute intervals into the arterial side of the extracorporeal
circulation.
After 30 minutes the cannulae were withdrawn and the vessels were sutured with No. 00000 silk. A heparin antagonist, hexadimethrine bromide (2.5 mg./kg.) was given intravenously
over a ten-minute period.
Chemical
Alkaline phosphatase activity.-The serum activity was measured
by the method of King (1951).
Estimation of Epodyl in blood.-This was measured by the colour reaction with p-hydroxy-azobenzene-p-sulphonic acid (Duncan and Snow, 1962).
Clinical Cases
A complete
history was usually avai-lable and a full clinical examination was made of the dogs admitted to the
Veterinary Hospital.
In most cases the dogs showed evidence of pain when the tumour was palpated. The circumference of the affected limb at the point of maximum swelling was measured and radiographs were made of the limb and the chest. In most dogs all the bones were radiographed. Arteriographs were occasionally made and, as well as showing the vascularity, were
of some value in
diagnosis (Owen and Stevenson,
1961).
Because of the high risk of metastatic spread biopsies were rarely taken before treatment was given but all cases were eventually confirmed as malignant tumours either by later biopsy or
post-mortem examination.
Haematological examination and serum alkaline phosphatase estimations were done in all cases. In some dogs serum transaminases were estimated and the serum proteins studied by
electrophoresis.
Experimental dogs without tumours were occasionally used to obtain information which could not ethically
be obtained from clinical cases.
RESULTS
Intra-arterial
injection Five dogs with osteosarcomas were treated by intra-arterial injections (Table I). In two dogs there was abolition of pain, post-injection oedema and regression of the tumour, but one of these dogs which was in poor condition and which had
a very large
tumour died a week later. The other dog showed changes in the radiographic appearance of the affected metacarpal bone with resorption of periosteal new bone. In this case 50 mg. of cyclophosphamide was given orally daily to try to prevent tumour recurrence. Five weeks after the Epodyl injection the dog chewed its own leg in half at the tumour site and, at the owner's request, was painlessly killed.
TABLE I.-Intra-arterial Epodyl

Only temporary arrest of growth occurred in a sarcoma of the distal ulna in a mongrel. The oral administration of cyclophosphamide appeared to have little effect and following limb amputation thioTEPA (triethylene-thiophosphoramide) given intramuscularly did not prevent the rapid appearance of lung metastases. In a Borzoi Epodyl was given by slow intra-arterial drip over 90 minutes daily for 5 days but a
total dose of 230 mg./kg. proved to be toxic and the animal died from tubular necrosis of the kidneys.
Occlusion of the Aorta
Before treating clinically affected dogs some experiments were performed on normal dogs under general anaesthesia.
During the development
of the method of occlusion, braided nylon loops were at first placed around the coeliac axis and around the aorta just posterior to the coeliac axis. Both vessels were occluded and Epodyl then injected into the cephalic vein. It was expected that following release of the
occluded coeliac axis there would be a rapid fall in the concentration of Epodyl in the blood as the drug was detoxicated in the liver. This did not occur. In later experiments and in the clinical cases treated the aorta alone was occluded at a point just cranial to the coeliac
artery.
When the aorta was occluded in
two dogs
and 10
ml. of sulphan
blue (6-2 per cent w/v) injected into the cephalic vein, rapid colouration of the skin in the anterior half of the body was observed followed several minutes later by a paler blue colouration posteriorly. Ten minutes after injection of the dye the dogs were killed with the aorta still occluded and it was found that there was deep blue colouration of the lungs, no obvious dye in the kidneys but some dye in the intestines. The bone marrow in the vertebrae anterior to the aortic occlusion was deep blue but posteriorly was hardly
coloured.
The main collateral channel to the posterior part of the body in the dog is the internal thoracic artery (Fig. 3) which supplies blood via the
superficial and deep epigastric arteries and the musculo-phrenic arteries. Temporary occlusion of
blood flow in the internal thoracic vessels could not be achieved without major surgery. Small quantities of blood may also be carried by the oesophageal part of the broncho-oesophageal artery and by the anastomosis of dorsal segmental arteries. The ventral spinal artery may theoretically be considered a collateral pathway but its diameter is so small that it is of practically no
significance.
Results of experiments designed to estimate the quantity of Epodyl in the blood in the anterior half of the body compared with the posterior were very variable. However it appeared reasonably certain that 2 minutes after injecting the drug into the cephalic
vein with the aorta occluded the concentration in the jugular vein was at least twice the concentration in blood taken from the femoral artery. Even without aortic occlusion however concentrations in jugular blood were found to be higher than in the posterior vena cava.
In one dog Epodyl at a dose of 150 mg./kg. was injected into the cephalic vein with the aorta occluded. After ten minutes, pressure on the aorta
was
released. This dose, wThich when iinjected intravenouslv inlto a iiormal dog produces Ino
obvious effect upon the lungs, caused severe lung oedema and death in
24 hours.
The aorta in 2
dogs was
occluded 3
times a
week for 2
wNeeks and small doses of Epodyl injected into
the cephalic veini. Post-mortem examinationi showed nio thrombus formationi in the
aorta aind only slight damage to the vessel was caused bv the
nylon.
The details of :3 clinical cases are given in Table II. Only one dog,
a St.
Bernard affected bilaterally in the proximal humerus,
showed tumour regression but this was very striking in that pressure on the radial nerve was reduced and
the dog regained the full use of its paralysed right limb. Estimations of serum transaminases SGO/T and SGP/T were made in this dog and showed no great changes following injections of Epodyl. Iodine and takata-ara liver function tests showed no evidence of liver damage and little change in serum bilirubin values occurred. Within 2 weeks of therapy the serum albumin-globulin ratio had changed from 1: 2-2
to 1: 1-4 a reversal of the decline in serum albumin found in advanced progressive cancer.
Fi(-. 3. Diagramn showinig the main collater-al
vessels to the ahdomen aii(l lelvis of the dog.
The iiiternal thoiacic artery leaves the aniterior aorta aIn(d later (livi(des into the superficial
aid
dleep craniial epigastric arteries.

TABLE II. Injections of Epodyl after Clamping of Aorta

A bull terrier with osteosarcoma of the ribs was give repeated injections into
the anterior aorta via a catheter passed up the femoral artery. By injecting sulphan blue before injecting Epodyl the exact distribution to the affected ribs could be seen. No skin colouration occurred posterior to the occluded aorta. There was abolition of the very severe pain in this dog but only very temporary arrest of growth of the tumour.
In an Irish Setter aortic occlusion did not prevent death from bone marrow failure after a dose of 250 mg./kg. of Epodyl given over a 3-day period.
Isolated limb perfusion
From studies on
normal dead dogs it was found that the weight of a hind limb below the level of the tourniquet was about
7-9 per cent of the total body weight and the weight of a fore limb 3-5 per cent. Much of the weight of
the fore limb was bone.
The protocols of the 9 cases
treated by perfusion was given in Table III. Four hind limbs were perfused and five fore limbs: one of the
fore limbs was perfused on two occasions. The dose per kg. of perfused tissue varied from 600-800 mg. in hind limbs and 100-240 mg. in fore limbs. The total quantity of Epodyl added to the extra-corporeal circulation varied from 1-4
mg./ml.
The day following perfusion there was abolition of pain in the tumour area and in most cases a considerable degree of oedema in the treated limb. In three dogs with osteosarcomas (one distal tibia and two distal radius) there was oedema of the tumour followed by rapid necrosis. The oedema of the tumour area caused mechanical interference with the blood supply to the extremity and resulted in gangrene distal to the site of the tumour (Fig. 4). The limb between the point of cannulation and the tumour became oedematous and showed skin darkening but remained
viable.
In a St. Bernard and an Alsatian there was regression of osteosarcomas for 2 months and in a Great Dane (Case 7, Table III) for a period of 5 months. In this Great Dane, which lived 7 months after perfusion of Epodyl at a concentration of 1*3 mg. /ml., there was some
muscle atrophy of the affected limb and
partial
hair loss which was later replaced by white hair. The limb however could bear weight and no overextension of the carpus on the opposite forelimb occurred (Fig. 5). There was no radiographic
evidence of lung metastases.
FIG.
4.-Fore limb of St. Bernard (Case 5) showing the developing line of demarcation between
viable and dead tissue 12 days post perfusion.
FIG. 5.-Great Dane (Case 7) 44 months after perfusion. The
affected limb is
weight-bearing
but there is considerable muscle atrophy. The general condition of the dog is
good.

FiG. 6 (a), (b), (c).-X-rays of radius and ulna of Great Dane (Case 7) before perfusion and
2 and 44
months after perfusion.

TABLE III.-Tumours Treated by Perfusion of Epodyl

As well as regression assessed directly by measuring the circumference of the limb at the point of maximum tumour swelling, radiographic changes in tumour appearance occurred in the St. Bernard and Great Dane. There was resorption of periosteal new bone and a much smoother outline of the affected areas was apparent (Fig. 6). Recurrence was heralded by the proliferation of periosteal new bone.
An increase in serum alkaline phosphatase values was present the day after perfusion (Fig. 7). This was not solely a feature of osteosarcomas as an increased amount of the enzyme in the
blood also occurred when the limb of a dog
bearing a squamous cell carcinoma was perfused. A similar effect was seen when a normal dog and a nephrecto- mised dog
were perfused. An
increase in serum alkaline phosphatase occurred when an osteosarcoma was treated by radiotherapy.
Where therapy resulted in regression of osteosarcoma
and radiography showed resorption
of new bone
values fell below the pre-treatment figure, rising again soon after the tumour recurred (Fig. 7). There
was an expected
leucocytosis following perfusion but no depression of circulating
leucocytes below pre-treatment levels followed, indicating that little or no drug had entered the
systemic circulation.
FIG.
7.- The effects of perfusion of Epodvl on serum alkaline phosphatase values.

DISCUSSION'
In this series of
17 dogs with
malignant bone tumours, regression of the tumours following the use of Epodyl occurred in 12 dogs but was maintained
for 2 months
or more in only
five. The longest period of regression without evidence of lung metastases was 5 months. The very large
breed of dog seldom lives more than 10 years and this consequently represents about 4 per cent of the life span.
These results are poor compared with the results of treating osteosarcomas in man by high dosage supervoltage radiotherapy-where the 5-year survival rate was 25 per
cent (Westminster
Hospital, 1960). Nevertheless as some method must be found to treat the 75 per cent of human cases where radiotherapy fails and as radiotherapy in the dog has hitherto been unsuccessful,
attempts to treat dogs by the intra-arterial injection or perfusion of anti-tumour drugs are certainly
justified. The abolition of pain, possibly by the toxic action of Epodyl on sensory nerve endings, is a valuable
feature.
As expected, the best results
were obtained in the early small tumours. Unfortunately, all too often, affected dogs are not seen until very large tumours are present or metastasis has occurred. The prophylactic administration of
thioTEPA
and cyclophosphamide was not successful in preventing the
development of
lung metastases in two dogs when amputation was
performed after
considerable damage to the tumour had been
produced by Epodyl. At the present time there is little evidence
that drugs given " prophylactically " in
this way are
beneficial (Horwitz, 1960). It may be relevant that alkylating agents and
antimetabolites given in this way can lower the immune
reactions of the host.
Following perfusion the major toxic effect was considerable
oedema in the affected limb. This was a
direct effect of the drug as there was little or no postoperative oedema
in limbs of
normal dogs perfused with whole blood or mixtures of blood and dextran. When the distal radius or distal tibia was involved the oedema of the
tumour caused
pressure on the
vessels supplying the distal extremity of the
limb and resulted in gangrene of tissue
which was
already oedematous. Cyproheptadine
hydrochloride (10 mg.) injected intra-muscularly into two dogs post-perfusion produced no
obvious effect but larger doses included in the perfusion circuit combined with
anti-histaminic drugs may be of value. There is a belief that perfusion can
be improved by diluting the extra-corporeal blood with low molecular weight
dextrans as this material reverses any tendency of the red cells to sludge and improves co-axial flow
in the small
blood vessels (Sharp and Eggleton,
1963).
The use of papaverine as a vaso-dilatot
may not
be an
improvement. It dilates the normal vessels so that a greater quantity of blood
can be pumped
through the limb but its effect oIn the pathological vessels
supplying the tumour has not yet been determined. Abrams (1964) has recently shown in man that the vessels in a renal neoplasm did not
constrict in the same way as normal kidnev vessels when adrenaline was
injected into
the renal
artery.
It has been reported by Haller, Ransdell, Stowens and Rubel (1962) that in rare cases hexadimethrine bromide in large doses produced renal
toxic effects in man. Toxicity from this cause was not seen in the perfused dogs recorded
here which received recommended doses. It may be necessary in the future however
to use protamine
sulphate as a heparin antagonist until such time as the molecular size of hexadimethrine
can be better
stabilised.
The origin of the increased serum alkaline phosphatase following perfusion is of some interest. The serum activity is the resultant of two processes : (a) formation and liberation
of the enzyme by the tissues, especially the osteoblasts, and (b) its excretion by the liver. Increased
release into the
blood or impaired excretion would thus lead to a
raised serum level (Wilkinson, 1962). The increase after intra-arterial injection or perfusion of Epodyl is probably due to liberation of the enzyme from damaged osteoblasts in the limb. Any effect of
the drug on the liver is unlikely to play much part
as even in massive liver necrosis no dramatic rise in serum alkaline phosphatase activity
occurs.
Successful therapy resulted
in a gradual fall
in the
serum alkaline
phosphatase levels (Fig. 7). In two dogs the subsequent rise in levels indicating recrudescence
of the tumour occurred at the same time as clinical signs of regrowth (pain and swelling)
appeared.
SUMMARY
Seventeen dogs bearing spontaneous malignant tumours of bone were treated with the tumour inhibiting epoxide triethylene glycol diglycidyl ether (Epodyl). The drug was administered intra-arterially in five cases and by perfusion in 9
cases.
A technique for blocking the
aorta is described and was used in an attempt to limit the drug to the anterior half of the body in 3
dogs.
Regression of the tumours occurred in 12 dogs but was maintained for 2 months or more in only 5 of these. Radiographic changes occurred in the affected bones. The longest period of regression was 5
months.
Following perfusion there was
alleviation of pain in the tumour area. Oedema of the limb was the major toxic
effect and resulted in gangrene in four
cases.
Serum alkaline phosphatase
values rose rapidly after perfusion and in the more successful cases fell slowly to low values, rising
again at the time of tumour recurrence.
The
operations of limb perfusion were conducted jointly with Dr. P. Cliffe of the Westminster Children's
Hospital, and I am also indebted to him for encouragement and advice.
I wish to thank Dr. L. M. Cobb and Mr. I. H. Purchase for anaesthesia of most of the dogs and for help with the aorta block technique, and Prof. A. T. Phillipson and Dr. A. L. Walpole for advice on the manuscript.
Fig. 1 and 2 were drawn by Mr. H. D. Williamson and Fig. 3 by Mr. D. H. Steven.
Epodyl was supplied by I.C.I. (Pharmaceuticals) Ltd., Alderley Park, Macclesfield, Cheshire, and concentrations of Epodyl in blood were estimated by Dr. W. A. M. Duncan.
I am grateful to the Royal Society for a generous grant to purchase perfusion apparatus.
REFERENCES
ABRAMS, H. L.-(1964) Nature, Lond., 201, 167.
BOYLAND, E.,
STAUNTON, M. D. AND WILLIAMS, K.-(1961) Brit.
J. Cancer, 15, 498.
BRODEY, R. S., SAVER, R. M. AND MEDWAY, W.-(1963) J. Amer.
vet. med. Ass.,
143,
471.
CREECH, O., KREMENTZ, E. T., RYAN, R. F. AND WINBLAD, J. N.-(1958) Ann.
Surg., 148,
616.
DUNCAN, W. A. M. AND SNOW, G. A.-(1962) Biochem.
J., 8P.
HALLER, J. A., JNR., RANSDELL, H. T. JNR., STOWENS, D. AND RUBELL, W.
F.-(1962)
J. thorac. cardiov. Surg., 44, 486.
HORWITZ, H.-(1960) Brit. J.
Radiol., 33, 659.
IRFAN, M.-(1958)
'Studies on the
peripheral blood picture of the dog and cat in health and
disease.' Ph.D. thesis, p. 184-94. University of London.
KING, E. J.-(1951) 'Micro-analysis in Medical
Biochemistry'. London (J. &. A. Churchill), p. 56.
McCoy, J. R., ALLISON, J. B., CROSSLEY, M. L. AND WANNERMACHER, R. W.,
JNR.-
(1956) Amer. J. vet. Res., 17, 90. OWEN, L. N.-(1962)
Brit. J.
Cancer, 16, 441.
Idem AND
STEVENSON, D.
E.-(1961) Res.
vet. Sci., 2, 117.
RYAN, R. F.-(1960) 'Cancer chemotherapy.' Report No. 10, U.S. Dept. of Health
Education and Welfare, p. 47.
SHARP, A. A., EGGLETON, M. J.-(1963) J. clin. Path., 16, 551. SILVER, I. A.-(1964) Acta
radiol. Stockh. In Press.
WESTMINSTER HOSPITAL.-(1960) Rep. Brit. Emp. Cancer Campgn, 38, 328. WILKINSON, J. H.-(1962) 'An
Introduction to Diagnostic Enzymology.' London (Edward Arnold (Publishers) Ltd.),
p.
85.
Share this article / Teilen Sie diesen Artikel